
More Information
Submitted: June 05, 2026 | Accepted: June 20, 2026 | Published: June 22, 2026
Citation: Jasuja S, Hiremath S, Nagaraju SP, Balwani M, Pasari A, Bhojaraja MV, et al. Clinico-epidemiological Profile, Comorbidities, Prevailing Practices in the Management of Hyperuricemia and Patient Outcomes with Various Urate Lowering Therapies: Capital Registry Data. J Clini Nephrol. 2026; 10(6): 50-57. Available from:
https://dx.doi.org/10.29328/journal.jcn.1001176
DOI: 10.29328/journal.jcn.1001176
Copyright license: © 2026 Jasuja S, et al. This is an open access article distributed under the Creative Commons Attribution License, which permits unrestricted use, distribution, and reproduction in any medium, provided the original work is properly cited.
Keywords: Chronic kidney disease; eGFR; Hyperuricemia; Serumuric acid

Clinico-epidemiological Profile, Comorbidities, Prevailing Practices in the Management of Hyperuricemia and Patient Outcomes with Various Urate Lowering Therapies: Capital Registry Data
Sanjiv Jasuja1, Sanjeev Hiremath2, Shankar Prasad Nagaraju3, Manish Balwani4, Amit Pasari4, Mohan V Bhojaraja3, Yogesh Sharma5*, Deepa Sholapuri5, Shivani Acharya5 and Rhutuja Rane5
1Indraprastha Apollo Hospital, New Delhi, India
2Sanjeev Clinic, 22nd Cross Road, Banashankari, StageII, Bengaluru, Karnataka, 560070 India
3Department of Nephrology, Kasturba Medical College, Manipal Academy of Higher Education, Manipal, India
4Saraswati Kidney Care Center (A unit of SS Multispeciality Hospital), Nagpur, 440015 Maharashtra, India
5Department of Medical Affairs, Abbott Healthcare Private Limited, Mumbai, 400 051, Maharashtra, India
*Corresponding author: Dr. Yogesh Sharma, Senior Medical Advisor, Medical Affairs, Abbott Healthcare Private Limited, Floor 16, Godrej BKC, Plot No. C – 68, BKC, Near MCA Club, Bandra (E) Mumbai – 400 051, Maharashtra, India, Email: [email protected]
Background: The absence of standardized protocols for managing hyperuricemia (HU) in chronic kidney disease (CKD) patients in India highlights the need to examine current practices. This registry assessed clinico-epidemiological data, treatment strategies, and outcomes with urate-lowering drugs (ULD) in CKD stages 2 to 4 across India.
Methods: This observational registry included 251 CKD patients with HU across five centers over 12 months. Primary endpoints were demographic data, CKD stages, and comorbidities. Secondary endpoints included percentages of patients on treatment (ULD, lifestyle modification [LSM], or both) and their impact on kidney function tests (KFTs). Comparisons were made between therapies (LSM vs. LSM+ULD) and comorbidity subgroups.
Results: Among 251 CKD patients, 48.6% had stage 4 CKD, and 58.2% had SUA levels 6-8 mg/dL (mean age: 46.77 years; 69.7% men). Hypertension (90%) was most common, followed by diabetes (41%).
At 12 months, mean SUA reduction was significant (-2.36 ± 1.85). Similar reductions occurred in patients with comorbidities: diabetes (-2.52 ± 1.83), hypertension (-2.39 ± 1.86), diabetes + hypertension (-2.51 ± 1.84) and others (-2.83 ± 2.06). Reduction was greater in patients treated with LSM+ULD (-2.89 ± 1.64) compared to LSM alone (-0.62 ± 1.69).
A significant eGFR increase was noted overall, with ULD+LSM group showing higher eGFR (15.21 ± 25.61) than LSM-only group (-1.26 ± 10.41). Seventeen adverse events (AEs) and three serious AEs were reported, all except one were unrelated.
Conclusion: The study highlights younger onset, male predominance, and higher ULD use in Indian CKD patients with hyperuricemia, supporting potential benefit of ULD+LSM in the management of CKD.
Hyperuricemia (HU) is defined as increased serum uric acid (SUA) levels exceeding the saturation level of 6.8 mg/dL at 370 C and pH 7 [1]. It may be symptomatic (gout, urolithiasis, acute urate nephropathy) or asymptomatic (elevated SUA without symptoms) [2]. HU is strongly associated with chronic kidney disease (CKD), hypertension (HTN), type 2 diabetes (T2DM), obesity, heart failure, and cardiovascular disease (CVD) [3]. It is also a mortality indicator in individuals with coronary artery disease, chronic obstructive pulmonary disease, and terminal cancers [4]. Multiple studies have confirmed elevated SUA as an independent risk factor of CVD incidence and mortality [5,6].
HU results from increased uric acid synthesis, reduced excretion, or both. About one-third of SUA originates from dietary purines, while the rest is endogenous [7].
Over the past 40 years, HU prevalence has gradually increased worldwide, with India reporting ~25.8%. [8,9]. Management includes lifestyle modifications and urate lowering drugs (ULDs).
KDIGO guidelines recommend intervention for symptomatic HU [10]. Dietary modifications such as limiting fructose, sugar-sweetened beverages, and red meat, may delay CKD progression. ULD like allopurinol also delay disease progression [11,12]. They are recommended for CKD, diabetes, CVD, heart failure patients to reduce mortality.
Updated recommendations from the American College of Rheumatology (ACR) [13]. The British Society for Rheumatology [14] and Japanese Guidelines [15] recommend using ULDs in asymptomatic HU only with added risk factors like CKD (especially stages 2-4).
However, there is no global consensus on how to treat asymptomatic HU. Further research on long-term ULD effects in high risk populations is needed [13]. Studies involving CKD patients on ULD have shown varying results, likely due to small sample sizes, brief follow-up, heterogeneous study designs, and varying CKD definitions.
Although current CKD guidelines do not prescribe treating HU without gout, emerging recognition supports a causative link [16,17]. Japanese guidelines partially recommend ULDs for HU patients with CKD to prevent deterioration of renal function, but not in hypertension or heart failure [15].
Primary urate-lowering therapy involves xanthine oxidase inhibitors like allopurinol or febuxostat. Allopurinol therapy can cause Stevens-Johnson syndrome as a side effect. Febuxostat is a non-purine xanthine oxidase inhibitor, is not associated with Stevens-Johnson- syndrome; it does not require dose adjustment in CKD. It may lower SUA levels more effectively [18].
Despite extensive literature on uricostatic and uricosuric medications, treatments given alter with time. Data on Indian CKD patients with HU remain minimal, particularly regarding clinico-epidemiological and treatment patterns. This study prospectively monitored HU in India, assessing prevalence, demographics, comorbidities, SUA levels, treatment and renal function patterns. Findings aim to guide medical professionals in tailoring optimal treatment strategies for patients with HU and other comorbidities.
Study design
This was a non-interventional, multi-centre, prospective observational registry study conducted across five sites in India. The study aimed to evaluate the prevalence of HU in CKD patients and to assess clinical characteristics, comorbidities, and patient demographics, and existing therapeutic strategies. The patients were followed for 12 months to evaluate disease progression and treatment impact. The data was categorized according to patients’ therapies (patients on LSM or ULD) and across comorbidities (DM, HTN, DM+HTN and others).
The Institutional Ethics Committee of all five study sites examined the clinical study protocol and other study documents and provided the approval letter to conduct the study. Every patient provided written informed consent before enrolment.
Setting
Eligible patients were recruited from outpatient departments at Sanjeev Clinic, Bengaluru; Apollo Hospital, New Delhi; Rukmini Hospital, Jaipur; Kasturba medical college, MAHE, Manipal, and Saraswati Kidney Care Centre, Nagpur. Patients were requested to attend follow- up visits at 3, 6 and 12 months for data collection. The study period extended from 23 JUL 2021 to 19 OCT 2023.
Eligibility criteria
Patients aged 18 to 65 years with CKD stages 2, 3A, 3B, or 4 (as per CKD Clinical Practice Recommendations for Primary Care Physicians and Healthcare Providers) and elevated SUA levels (> 7 mg/dL [420 µM] in males and > 6 mg/dL [360 µM] in women) were included.
Exclusion criteria included patients with a reduced life expectancy (e.g., < 6 months); recent conditions impairing participation, pregnant or lactating women, patients requiring long-term glucocorticoids, or with severe infections (excluding diabetic foot) or immune dysfunction.
The planned study duration was 24 months. However, it was terminated early at 12 months due to the dropout rate at later follow-up visits. Up until then, sufficient data was also acquired. Data of 251 eligible patients were collected. They were followed up at regular intervals [3 months (172 subjects), 6 months (154 subjects) and 12 months (138 subjects) (Figures 1,2).
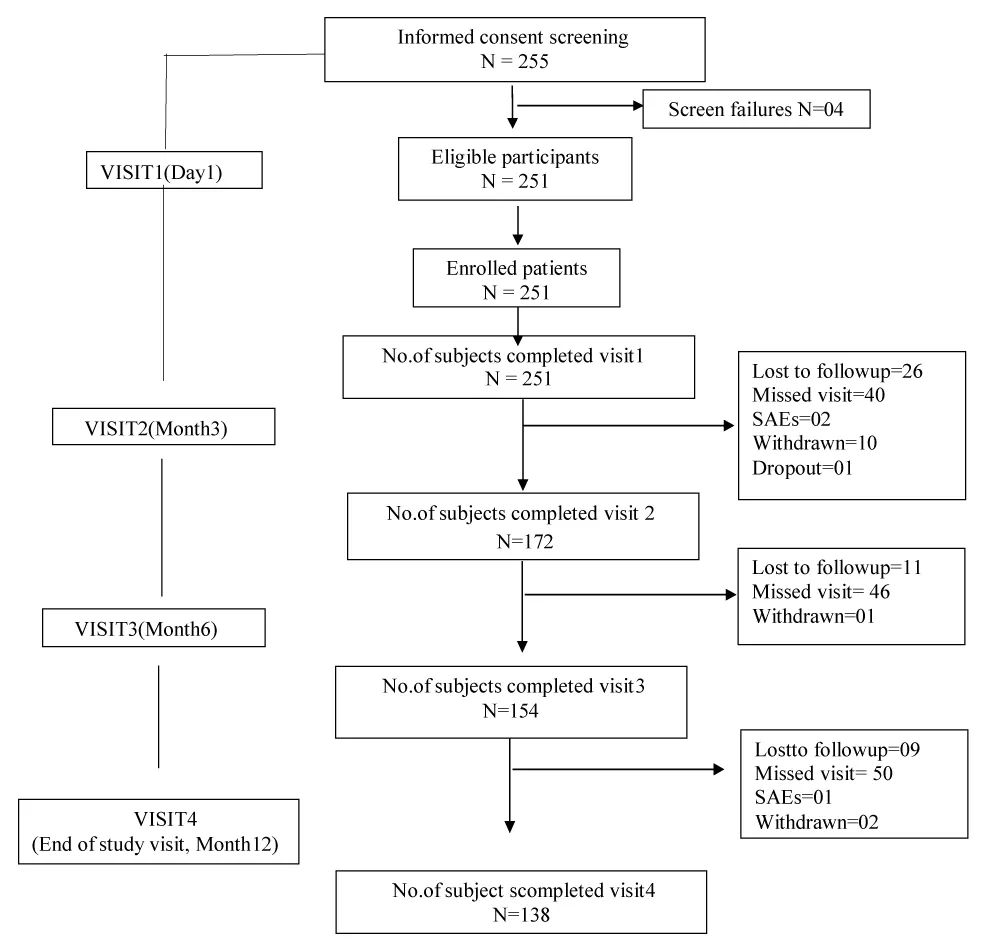
Figure 1: Patient disposition.
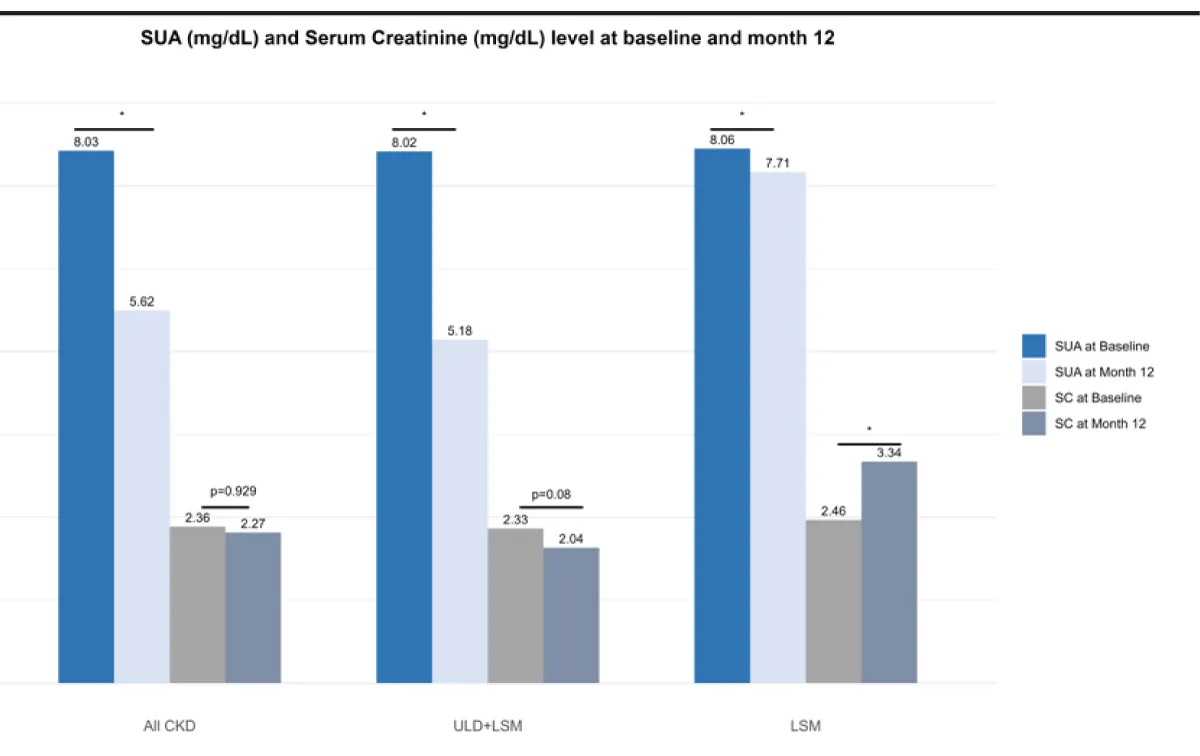
Figure 2: Change in SUA and serum creatinine from baseline to 12 months. CKD: Chronic Kidney Disease; ULD: Urate-Lowering Drug; LSM: Lifestyle Modification; SUA: Serum Uric Acid; SC: Serum Creatinine.
Study endpoints
The primary endpoint of the study was to check prevalence of HU with stage 2-4 along with collection of demographic data and clinical characteristics, including the percentage of CKD patients as per duration (≤ 2 years, 2–5 years, > 5 years) and percentage of CKD patients with SUA levels (6-8 mg/dL, 8-10 mg/dL and >10 mg/d) at baseline with HU and comorbidities. Secondary end points included the impact of HU treatment on KFT parameters over time, categorized by treatment group (ULD+LSM and LSM) and by comorbidities (DM, HTN, DM+HTN, and other conditions).
Study assessments
Patients’ demographic and baseline data, anthropometric data, medical/surgical history including CKD and comorbidities were collected during screening. Follow-up assessments included detailed documentation of KFT parameters, treatment adherence, comorbidity status and any concomitant medications. Changes in these parameters were analyzed statistically from baseline to 3, 6, and 12 months.
Bias
To minimize bias, data was captured prospectively in compliance with standard clinical trial processes to reflect real-world settings. The study employed a multi-centric deign with sites from different geographical locations. Additionally, analyses were stratified by treatment and comorbidity groups to reduce confounding.
Study size
The study was observational and exploratory in nature. Thus, no formal sample size calculation was performed. A total of 251 patients who met the eligibility criteria and consented were included, which was further considered sufficient to provide descriptive insights into study endpoints.
Statistical analysis
All collected data from the enrolled patients obtained as per protocol were used for summary/analysis. Considering extended duration of the follow-up study, data analysis and reporting were divided into two steps: once 50% of the subjects completed the study (with a 6- month follow-up) and again after 100% of the subjects completed the study (with a 12-month follow-up). Continuous variables were summarized using descriptive statistics such as n, mean, standard deviation, median, minimum and maximum values. Categorical data were summarized using numbers, percentages, and 95% confidence intervals. Missing data was not imputed.
Statistical tests were conducted at a 5% level of significance. For change from baseline summaries, the baseline value was the value recorded during the baseline visit. Statistical analysis was carried out with SPSS version 29.0.0.0 and R version 4.3.2. Paired t test was used for analyzing changes in KFT parameters from baseline to 3, 6 and 12 months.
Patient demographics and baseline characteristics
a. Demographics
A total of 251 eligible patients were enrolled. Baseline demographics are presented in Table 1.
| Table 1: Patient demographics | |
| Characteristics | Overall (N=255) |
| AGE | |
| N | 251 |
| Mean | 46.77 |
| SD | 49.00 |
| Median | 11.53 |
| Min; Max | (19, 65) |
| GENDER, n (%) | |
| Female | 76 (30.3%) |
| Male | 175 (69.7%) |
| ANTHROPOMETRY Weight (kg) | |
| N | 251 |
| Mean | 69.58 |
| SD | 68 |
| Median | 14.98 |
| Min; Max | (37.81 116.2) |
| Height (m) | |
| N | 251 |
| Mean | 163.75 |
| SD | 163 |
| Median | 8.96 |
| Min; Max | (139.7, 190.0) |
| BMI (kg/m2) | |
| N | 251 |
| Mean | 25.89 |
| SD | 25.64 |
| Median | 4.93 |
| Min, Max | (15.8, 47.2) |
| ETHNICITY, n (%) | |
| Indian | 251 (100.0%) |
| EDUCATION CATEGORIES n (%) | 251 (100.0%) |
| Illiterate | 6 (2.4%) |
| Primary school certificate | 7 (2.8%) |
| Middle school certificate | 32 (12.8%) |
| High school certificate | 58 (23.1%) |
| Intermediate or diploma | 19 (7.6%) |
| Graduate | 117 (46.6%) |
| Profession | 12 (4.8%) |
| OCCUPATION, n (%) | 251 |
| Unemployed | 83 (33.1%) |
| Elementary occupation | 18 (7.2%) |
| plant and machine operators/assemblers | 10 (4.0%) |
| Craft & related trade workers | 6 (2.4%) |
| Skilled agricultural/fishery workers | 14 (5.6%) |
| Skilled workers/shop and market sales workers | 40 (15.9%) |
| Clerks, technicians/associate professionals | 20 (8.0%) |
| Professionals | 52 (20.7%) |
| Legislators/senior officials/manager | 8 (3.2%) |
| LIFESTYLE HABITS | |
| Smoking, n (%) | |
| Current | 15 (6.0%) |
| Former | 19 (7.6%) |
| Never | 217 (86.5%) |
| Alcohol consumption, n (%) | |
| Current | 25 (10.0%) |
| Former | 25 (10.0%) |
| Never | 201 (80.0%) |
| Dietary habits, n (%) | |
| Vegetarian | 109 (43.4%) |
| Both Vegetarian & Non-vegetarian | 142 (56.6%) |
| SD: Standard Deviation; N: Total number; n: number in the category | |
b. Baseline characteristics
1. CKD stage, duration and SUA level
Among 251 patients, 122(48.6%) had stage 4 CKD, 49 (19.5%) had stage 3B, 42 (16.7%) stage3A and 38 (15.1%) stage 2. Baseline SUA levels were 6-8 mg/dL in 58.2%, 8-10 mg/dL in 35.5%, and >10 mg/dL in 6.4%. Most patients (44.2%) had CKD for ≤ 2 years, while 31.9% had > 5 years (Table 2).
| Table 2: Percentage of CKD patients withhyperuricemiaby CKD stages, duration,SUA level and comorbidities. | ||||
| Characteristics | ULD + LSM (N=199) | Lifestyle modification (N=52) | Overall (N=251) | |
| CKD stages | HU (SUA level), n (%) | |||
| 2 | 6–8 mg/dL | 22 (11.1%) | 3 (5.8%) | 25 (10.0%) |
| 8–10 mg/dL | 12 (6.0%) | 1 (1.9%) | 13 (5.2%) | |
| >10 mg/dL | 0 (0.0%) | 0 (0.0%) | 0 (0.0%) | |
| 34 (17.1%) | 4 (7.7%) | 38 (15.1%) | ||
| 3A | 6–8 mg/dL | 20 (10.1%) | 3 (5.8%) | 23 (9.2%) |
| 8–10 mg/dL | 13 (6.5%) | 4 (7.7%) | 17 (6.8%) | |
| >10 mg/dL | 2 (1.0%) | 0 (0.0%) | 2 (0.8%) | |
| 35 (17.6%) | 7 (13.5%) | 42 (16.7%) | ||
| 3B | 6–8 mg/dL | 25 (12.6%) | 5 (9.6%) | 30 (11.9%) |
| 8–10 mg/dL | 9 (4.5%) | 3 (5.8%) | 12 (4.8%) | |
| >10 mg/dL | 5 (2.5%) | 2 (3.8%) | 7 (2.8%) | |
| 39 (19.6%) | 10 (19.2%) | 49 (19.5%) | ||
| 4 | 6–8 mg/dL | 50 (25.1%) | 18 (34.6%) | 68 (27.1%) |
| 8–10 mg/dL | 36 (18.1%) | 11 (21.2%) | 47 (18.7%) | |
| >10 mg/dL | 5 (2.5%) | 2 (3.8%) | 7 (2.8%) | |
| 91 (45.7%) | 31 (59.6%) | 122 (48.6%) | ||
| Duration of CKD | ||||
| ≤ 2 years | 72 (36.2%) | 39 (75.0%) | 111 (44.2%) | |
| 2–5 years | 53 (26.6%) | 7 (13.5%) | 60 (23.9%) | |
| > 5 years | 74 (37.2%) | 6 (11.5%) | 80 (31.9%) | |
| SUA Levels | ||||
| 6–8 mg/dL | 117 (58.8%) | 29 (55.8%) | 146 (58.2%) | |
| 8–10 mg/dL | 70 (35.2%) | 19 (36.5%) | 89 (35.5%) | |
| >10 mg/dL | 12 (6.0%) | 4 (7.7%) | 16 (6.4%) | |
| Comorbidities | ||||
| DM | 74 (37.2%) | 29 (55.8%) | 103 (41.0%) | |
| HTN | 179 (89.9%) | 47 (90.4%) | 226 (90.0%) | |
| DM + HTN | 70 (35.2%) | 26 (50.0%) | 96 (38.2%) | |
| Other comorbidities | 70 (35.2%) | 11 (21.2%) | 81 (32.3%) | |
2. Comorbidities
Majority of the patients had HTN (90.0%), followed by DM (41.0%), DM+HTN (38.2%) and other comorbidities (32.3%) (Table 2).
3. Treatment distribution
At baseline, 79.3% received ULD+ LSM, 20.7% were on LSM alone. By the end of study, the proportion of patients on ULD+LSM increased to 82.6% (Table 3).
| Table 3: Summary of CKD patients on hyperuricemia treatment. | ||
| Characteristics | Visit | Values |
| HU treatment | ||
| Visit-1 | ||
| N | 251 | |
| Urate lowering drugs, n (%) | 199(79.3%) | |
| Febuxostat, n (%) | 196 (78.1%) | |
| Topiroxostat, n (%) | 3 (1.2) | |
| Lifestyle modification, n (%) | 52(20.7%) | |
| Visit-2 | ||
| N | 172 | |
| Urate lowering drugs, n (%) | 130(75.6%) | |
| Febuxostat, n (%) | 127 (73.8%) | |
| Topiroxostat, n (%) | 3 (1.7%) | |
| Lifestyle modification, n (%) | 42(24.4%) | |
| Visit-3 | ||
| N | 154 | |
| Urate lowering drugs, n (%) | 121(78.6%) | |
| Febuxostat, n (%) | 118 (76.6%) | |
| Topiroxostat, n (%) | 3 (1.9) | |
| Lifestyle modification, n (%) | 33(21.4%) | |
| Visit-4 | ||
| N | 138 | |
| Urate lowering drugs, n (%) | 114(82.6%) | |
| Febuxostat, n (%) | 111 (80.4) | |
| Topiroxostat, n (%) | 3 (2.2) | |
| Lifestyle modification, n (%) | 24(17.4%) | |
| Percentage is computed using N provided for each visit HU – Hyperuricemia. All patients were on lifestyle modification |
||
Impact of treatment on KFT parameters
In the overall CKD group, mean serum urea, creatinine, BUN decreased by month 12, though changes were not statistically significant.
The mean SUA decreased from 8.03 (1.2) at baseline to 5.62 (1.81) at Month 12, exhibiting a statistically significant reduction (p = < 0.001). Mean eGFR increased from 37.02(18.95) at baseline to 49.5(28.86) at month 12, also statistically significant (p < 0.001).
Across comorbidity subgroups, significant decrease in mean baseline readings of serum urea, serum creatinine, BUN were observed. Mean eGFR levels were found to be significantly higher (p = < 0.001) at month 12 in all these subgroups (Table 4).
| Table 4: Summary table of s. urea, s. creatinine, SUA, BUN and eGFR of overall CKD patients, urate lowering drugs + lifestyle modification and lifestyle modification alone population | |||||||||||||||||||||||||
| Mean (SD) | Change from baseline | ||||||||||||||||||||||||
| Visits ¢ |
Baseline | 3 months | 6 months | 12 months | Baseline | 3 months | p value | 6 months | p value | 12 months | p value | ||||||||||||||
| Overall CKD patients | |||||||||||||||||||||||||
| SU | 52.11 | 53.3 | 52.73 | 49.17 | - | 0.67 | 0.725 | -1.36 | 0.566 | -3.6 | 0.128 | ||||||||||||||
| ( ± 23.35) | ( ± 28.77) | ( ± 29.38) | ( ± 30.67) | ( ± 24.85) | ( ± 29.32) | ( ± 27.55) | |||||||||||||||||||
| SC | 2.36 | 2.3 | 2.36 | 2.27 | - | 0.03 | 0.682 | 0.03 | 0.769 | -0.01 | 0.929 | ||||||||||||||
| ( ± 0.98) | ( ± 1.29) | ( ± 1.55) | ( ± 1.83) | ( ± 0.98) | ( ± 1.35) | ( ± 1.53) | |||||||||||||||||||
| SP | 6.89 | 7.01 | 7.05 | 7.02 | - | 0.05 | 0.35 | 0.1 | 0.043* | 0.04 | 0.445 | ||||||||||||||
| ( ± 0.68) | ( ± 0.71) | ( ± 0.74) | ( ± 0.66) | ( ± 0.63) | ( ± 0.63) | ( ± 0.67) | |||||||||||||||||||
| SUA | 8.03 | 6.04 | 5.98 | 5.62 | - | 1.91 | <0.001* | 2.06 | <0.001* | 2.36 | <0.001* | ||||||||||||||
| ( ± 1.2) | ( ± 1.87) | ( ± 2.03) | ( ± 1.81 | ( ± 1.92) | ( ± 1.99) | ( ± 1.85) | |||||||||||||||||||
| BUN | 24.89 | 25.16 | 24.76 | 23.03 | - | 0.22 | 0.808 | 0.54 | 0.612 | -2.09 | 0.071 | ||||||||||||||
| ( ± 10.65) | ( ± 13.93) | ( ± 13.6) | ( ± 14.3) | ( ± 11.76) | ( ± 13.11) | ( ± 13.1) | |||||||||||||||||||
| eGFR | 37.02 | 42.2 | 44.35 | 49.5 | - | 4.95 | <0.001* | 8.82 | <0.001* | 12.35 | <0.001* | ||||||||||||||
| ( ± 18.95) | ( ± 23.7) | ( ± 25.94) | ( ± 28.86) | ( ± 15.93) | ( ± 20.99) | ( ± 24.47) | |||||||||||||||||||
| CKD patients receiving urate lowering drugs + lifestyle modification | |||||||||||||||||||||||||
| SU | 52.28 | 52.51 | 50.51 | 47.59 | - | -0.58 | 0.798 | -4.57 | 0.08 | -6.32 | 0.015* | ||||||||||||||
| ( ± 24.32) | ( ± 29.8) | ( ± 27.73) | ( ± 30.14) | ( ± 25.79) | ( ± 28.49) | ( ± 27.36) | |||||||||||||||||||
| SC | 2.33 | 2.25 | 2.15 | 2.04 | - | 0.03 | 0.748 | -0.13 | 0.226 | -0.22 | 0.08 | ||||||||||||||
| ( ± 1.02) | ( ± 1.35) | ( ± 1.36) | ( ± 1.56) | ( ± 1.06) | ( ± 1.2) | ( ± 1.3) | |||||||||||||||||||
| SP | 6.89 | 7.02 | 7.08 | 6.96 | - | 0.05 | 0.42 | 0.13 | 0.025* | 0.02 | 0.751 | ||||||||||||||
| ( ± 0.66) | ( ± 0.65) | ( ± 0.68) | ( ± 0.66) | ( ± 0.64) | ( ± 0.64) | ( ± 0.67) | |||||||||||||||||||
| SUA | 8.02 | 5.52 | 5.54 | 5.18 | - | -2.39 | <0.001* | -2.46 | <0.001* | -2.75 | <0.001* | ||||||||||||||
| ( ± 1.18) | ( ± 1.73) | ( ± 1.95) | ( ± 1.5) | ( ± 1.91) | ( ± 1.99) | ( ± 1.73) | |||||||||||||||||||
| BUN | 25.31 | 24.88 | 23.75 | 22.3 | - | -0.63 | 0.571 | -2.23 | 0.052 | -3.53 | 0.006* | ||||||||||||||
| ( ± 11.12) | ( ± 14.55) | ( ± 12.8) | ( ± 14.05) | ( ± 12.32) | ( ± 12.5) | ( ± 13.01) | |||||||||||||||||||
| eGFR | 38.31 | 44.92 | 47.75 | 52.9 | - | 6.01 | <0.001* | 11.43 | <0.001* | 15.21 | <0.001* | ||||||||||||||
| ( ± 19.59) | ( ± 24.88) | ( ± 26.36) | ( ± 29.09) | ( ± 17.68) | ( ± 21.9) | ( ± 25.61) | |||||||||||||||||||
| CKD patients treated only with lifestyle modification | |||||||||||||||||||||||||
| SU | 51.47 | 52.51 | 61.16 | 56.69 | - | 4.53 | 0.18 | 10.76 | 0.049* | 56.69 | 0.082 | ||||||||||||||
| ( ± 19.35) | ( ± 25.89) | ( ± 34.09) | ( ± 32.66) | ( ± 21.48) | ( ± 29.67) | ( ± 32.66) | |||||||||||||||||||
| SC | 2.46 | 2.45 | 3.15 | 3.34 | - | 0.03 | 0.756 | 0.65 | 0.036* | 0.96 | 0.036* | ||||||||||||||
| ( ± 0.87) | ( ± 1.05) | ( ± 1.95) | ( ± 2.54) | ( ± 0.68) | ( ± 1.69) | ( ± 2.11) | |||||||||||||||||||
| SP | 6.89 | 6.97 | 6.95 | 7.2 | - | 0.04 | 0.642 | -0.005 | 0.964 | 0.15 | 0.266 | ||||||||||||||
| ( ± 0.76) | ( ± 0.87) | ( ± 0.92) | ( ± 0.64) | ( ± 0.6) | ( ± 0.57) | ( ± 0.65) | |||||||||||||||||||
| SUA | 8.06 | 7.66 | 7.58 | 7.71 | - | -0.42 | 0.009* | -0.61 | 0.007* | -0.53 | 0.041* | ||||||||||||||
| ( ± 1.29) | ( ± 1.25) | ( ± 1.43) | ( ± 1.72) | ( ± 0.99) | ( ± 1.2) | ( ± 1.19) | |||||||||||||||||||
| BUN | 23.57 | 26.05 | 28.58 | 26.49 | - | 2.71 | 0.076 | 5.81 | 0.022* | 4.35 | 0.082 | ||||||||||||||
| ( ± 8.99) | ( ± 11.91) | ( ± 15.93) | ( ± 15.26) | ( ± 9.68) | ( ± 13.62) | ( ± 11.73) | |||||||||||||||||||
| eGFR | 32.06 | 33.79 | 31.5 | 33.33 | - | 1.69 | 0.17 | -1.07 | 0.652 | -1.26 | 0.56 | ||||||||||||||
| ( ± 15.41) | ( ± 17.3) | ( ± 19.83) | ( ± 22.25) | ( ± 7.82) | ( ± 13.27) | ( ± 10.41) | |||||||||||||||||||
| Note: SU: Serum Urea; SCp Serum Creatinine; SP: Serum Protein; BUN: Blood Urea Nitrogen; eGFR: estimated Glomerular Filtration Rate; p value based on paired t test; *Significant p value |
|||||||||||||||||||||||||
Subgroup analysis: ULD+LSM and LSM only
All subjects received LSM. Among those prescribed ULD received either Febuxostat (80.4%) or Topiroxostat (2.2%), remaining 17.4% patients were on LSM alone.
A statistically significant reduction in mean serum urea, SUA and BUN values was observed in ULD+LSM subgroup. On the contrary LSM only group showed increased mean serum urea and creatinine at month 12. Mean eGFR values increased significantly at month 12 compared to baseline in the ULD+LSM subgroup, whereas a decline was noted in the LSM only subgroup.
Intragroup comparisons confirmed significant reductions in serum urea, SUA, BUN, and a greater eGFR improvement in the ULD+LSM, compared to the patients on LSM alone at Month 12 (Table 4, Figure 3).
Safety
Seventeen adverse events (AEs) were reported by 13 patients, including 3 serious adverse events (SAEs). Only one AE was possibly related (ADR) to prescribed therapy.
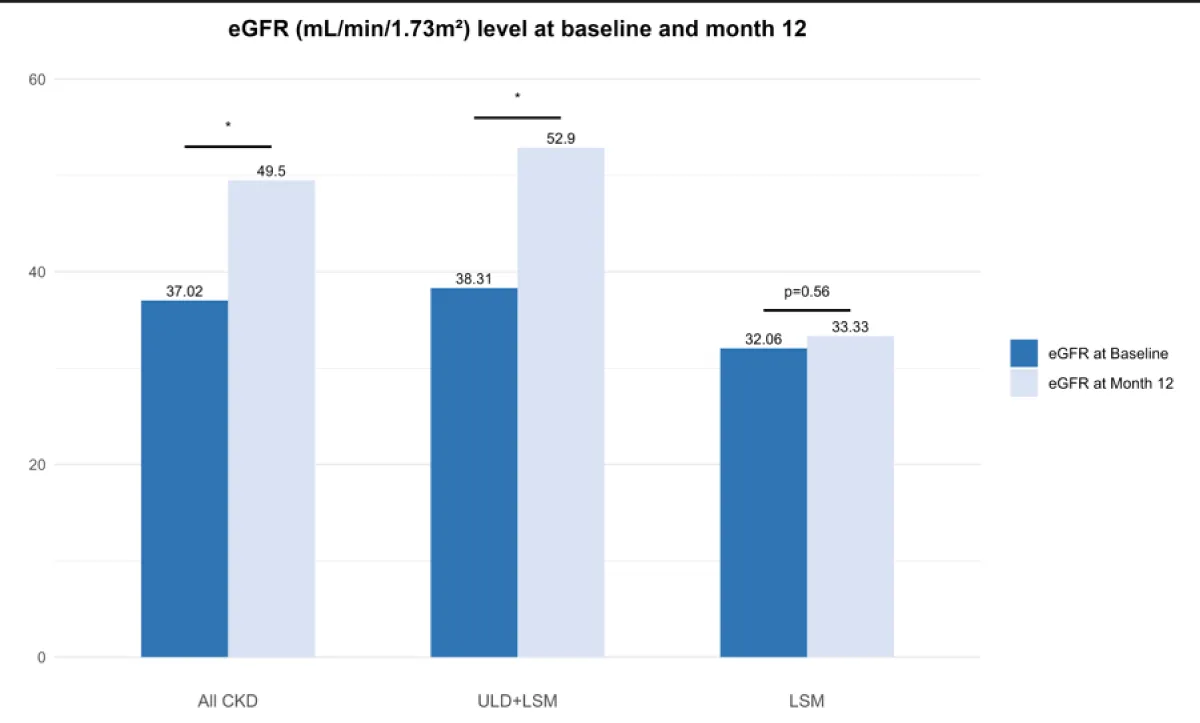
Figure 3: Changein eGFR level from baseline to 12 months. *p < 0.05 is considered as statistically significant. p - values are based on paired-t test. CKD: Chronic Kidney Disease; ULD: Urate-Lowering Drug; LSM: Lifestyle Modification; eGFR: estimated Glomerular filtration rate.
The loss of renal function in CKD is irreversible, but it can be delayed through management of nutritional and metabolic factors, thus slowing disease progression and improving life expectancy. This is important particularly in countries with limited access to renal replacement therapy [19]. In India, there are no clear guidelines for treating HU in CKD patients. Therefore, it is essential to explore prevailing practices across regions. Our study aims to address this gap by studying management strategies and outcomes in Indian CKD patients with elevated SUA.
Most enrolled patients had stage 4 CKD, with SUA levels between 6-8 mg/dL, and CKD < 2 years. HTN was the most common comorbidity, highlighting the need for targeting management strategies addressing elevated SUA levels and comorbidities. At baseline, ULD+LSM use was maximum, and increased further by study end. These findings emphasize the importance of establishing treatment protocols to manage HU and prevent CKD progression.
Several prospective studies stratified patients by SUA levels and revealed a favourable connection with CKD occurrence [20-24]. In a registry of 48,000 Japanese patients followed for 7 years, Iseki, et al. reported HU significantly increased the risk of end-stage kidney disease after controlling serum creatinine and other variables [25]. Similar trends were observed in National Health and Nutrition Examination Survey (NHANES) 2007–2008 analysis of 5,707 patients, which revealed an exponential SUA-CKD relationship [26]. A community study of 13,338 participants identified elevated UA level as an independent risk factor for CKD progression and mortality [27]. Prezelin-Reydit M, et al.
further emphasized the risk of kidney failure rises with SUA, plateauing at 6-10 mg/dl and increase sharply above 11 mg/dl [28].
In NHANES 2001-2018, HU with HTN was linked to increased risk of cardiovascular and all- cause mortality [29]. Collectively, these studies confirm SUA as a key factor in CKD progression and mortality, particularly in patients with comorbidities.
Our non-interventional, multicenter, observational study compared SUA changes in overall CKD patients and in those with comorbidities. Indicators of CKD progression, like SUA, eGFR, serum creatinine, blood urea etc., were analyzed. The current study demonstrated a statistically significant decrease in serum urea and SUA along with increased eGFR over 12- months, suggesting improved kidney function in both overall CKD and comorbidity subgroups (DM, HTN, DM+HTN, others).
Unlike LSM alone, patients on ULD+LSM showed significant increase in eGFR and decrease in serum urea, SUA and serum creatinine.
Weis L, et al. observed improved GFR was associated with a decrease in metabolic problems over time, indicating renal function improvement [30]. Traditionally eGFR is considered a more accurate measure of renal health than serum creatinine [31,32].
In current study, eGFR increased significantly in overall CKD patients, with ULD+LSM subgroup suggesting a slow progression of CKD than LSM alone. LSM patients displayed an insignificant declining eGFR trend.
Goicoechea, et al. [33] observed an inverse SUA-eGFR correlation. After 59 months of follow‑up in 900 healthy adults, higher SUA predicted greater eGFR reduction [34]. The findings of our observational study are consistent with the findings mentioned above.
A systematic MEDLINE review of randomized controlled trials comparing renal events in non- dialyzed CKD patients showed ULT tend to preserve eGFR better, though not significantly [35].
Enhanced kidney functioning with ULD+LSM implied significant improvements in eGFR and reductions in SUA, serum creatinine and BUN. Subgroup analysis clarified the therapeutic effects, though larger sample sizes are required to validate these results. The study employed real-world, multicenter data from five major Indian cities, increasing the representativeness of urban and semi-urban CKD populations, making the results more reflective of routine clinical practice.
Nevertheless, certain limitations stem from its observational nature, including varied laboratory acquisition, compliance problems and the inability to fully exclude bias. While the multicentre approach improves generalizability within urban India, rural and underserved populations remain underrepresented, limiting extrapolation.
Furthermore, the overall sample size of 251 patients, coupled with an imbalance in treatment distribution (79.3% in the HU treatment + LSM group and 20.7% in LSM-only group), limits the statistical power for subgroup analyses and reduces the likelihood of detecting rare outcomes. Despite these constraints, the findings add valuable real-time insights into HU management in Indian CKD patients, highlighting areas for further research.
The study highlights a higher preference for urate lowering drugs among Indian nephrologists. Additionally, Indian CKD patients with hyperuricemia tend to have a younger age onset with a greater prevalence in males. The findings of the study underscore the synergistic effects of combining urate-lowering medications with lifestyle modifications in improving renal function and mitigating the progression of the disease.
Acknowledgement
The authors acknowledge Ketham Karunakar Likitha, Lead Medical Writer at IDD Research Solutions for Medical Writing Support.
The authors also thank the entire IDD Research Solutions team for their contributions in Clinical Operations, Project Management, Data Management and Biostatistics.
Funding: This study was sponsored by Abbott Healthcare Pvt. Ltd.
Conflict of interest: Dr. Sanjiv Jasuja, Dr. Sanjeev Hiremath, Dr. Shankar Prasad & Dr. Manish Balwani, Dr. Amit Pasari, Dr. Mohan V Bhojaraja received research grants from Abbott for conduct of the study.
Dr. Yogesh Sharma, Dr. Deepa Sholapuri, Dr. Shivani Acharya, Dr. Rhutuja Rane are the employees of Abbott Healthcare Private limited.
Ethical approval: Institutional Ethics Committees (IEC) of each study site (ACE ICE, Royal Pune IEC, Kasturba Medical College and hospital IEC, Criti Care Hospital and research IEC and Apex Hospital IEC) reviewed and approved the clinical study protocol and other study- related documents. All patients provided written informed consent before their participation in the study.
- Pai BH, Swarnalatha G, Ram R, Siva Kumar V. Allopurinol for prevention of progression of kidney disease with hyperuricemia. Indian J Nephrol. 2013;23(4):280-6. Available from: https://doi.org/10.4103/0971-4065.114499
- Dincer HE, Dincer AP, Levinson DJ. Asymptomatic hyperuricemia: to treat or not to treat. Cleve Clin J Med. 2002;69(8):594, 597, 600-2. Available from: https://doi.org/10.3949/ccjm.69.8.594
- Richette P, Perez-Ruiz F, Doherty M, Jansen TL, Nuki G, Pascual E, et al. Improving cardiovascular and renal outcomes in gout: what should we target? Nat Rev Rheumatol. 2014;10(11):654-61. Available from: https://doi.org/10.1038/nrrheum.2014.124
- Zhang X, Liu L, Liang R, Jin S. Hyperuricemia is a biomarker of early mortality in patients with chronic obstructive pulmonary disease. Int J Chron Obstruct Pulmon Dis. 2015;10:2519-23. Available from: https://doi.org/10.2147/copd.s87202
- Kleber ME, Delgado G, Grammer TB, Silbernagel G, Huang J, Krämer BK, et al. Uric acid and cardiovascular events: a Mendelian randomization study. J Am Soc Nephrol. 2015;26(11):2831-8. Available from: https://doi.org/10.1681/asn.2014070660
- Freilich M, Arredondo A, Zonnoor SL, McFarlane IM. Elevated serum uric acid and cardiovascular disease: a review and potential therapeutic interventions. Cureus. 2022;14(3):e23625. Available from: https://doi.org/10.7759/cureus.23582
- George C, Leslie SW, Minter DA. Hyperuricemia. In: StatPearls [Internet]. Treasure Island (FL): StatPearls Publishing; 2023 [cited 2024 Aug 6]. Available from: https://www.ncbi.nlm.nih.gov/books/NBK499945/
- Global prevalence of hyperuricemia: a systematic review of population-based epidemiological studies [Internet]. American College of Rheumatology; 2015 [cited 2024 Aug 6]. Available from: https://acrabstracts.org/abstract/global-prevalence-ofhyperuricemia-a-systematic-review-of-population-based-epidemiological-studies/
- Billa G, Dargad R, Mehta A. Prevalence of hyperuricemia in Indian subjects attending hyperuricemia screening programs-a retrospective study. J Assoc Physicians India. 2018;66(4):43-6.
- Levin A, Baumgartner L, Coresh JJ, Foster B, Francis A, Hall RK, et al. Executive summary of the KDIGO 2024 Clinical Practice Guideline for the Evaluation and Management of Chronic Kidney Disease: known knowns and known unknowns. Kidney Int. 2024;105(4):684-701. Available from: https://doi.org/10.1016/j.kint.2023.10.016
- Choi HK, Liu S, Curhan G. Intake of purine-rich foods, protein, and dairy products and relationship to serum levels of uric acid: the Third National Health and Nutrition Examination Survey. Arthritis Rheum. 2005;52(1):283-9. Available from: https://doi.org/10.1002/art.20761
- Siu YP, Leung KT, Tong MK, Kwan TH. Use of allopurinol in slowing the progression of renal disease through its ability to lower serum uric acid level. Am J Kidney Dis. 2006;47(1):51-9. Available from: https://doi.org/10.1053/j.ajkd.2005.10.006
- Gout treatment guidelines [Internet]. Arthritis Foundation; [cited 2024 Aug 6]. Available from: https://www.arthritis.org/diseases/more-about/gout-treatment-guidelines
- Hui M, Carr A, Cameron S, Davenport G, Doherty M, Forrester H, et al. The British Society for Rheumatology Guideline for the Management of Gout. Rheumatology (Oxford). 2017;56(7):1056-9. Available from: https://doi.org/10.1093/rheumatology/kex156
- Hisatome I, Ogino K, Kotake F. Japanese Society of Gout and Uric & Nucleic Acids 2019 Guidelines for Management of Hyperuricemia and Gout 3rd edition. Gout Uric Nucleic Acids. 2020;44:1-37.
- Sato Y, Feig DI, Stack AG, Kang DH, Lanaspa MA, Ejaz AA, et al. The case for uric acid-lowering treatment in patients with hyperuricaemia and CKD. Nat Rev Nephrol. 2019;15(12):767-75. Available from: https://doi.org/10.1038/s41581-019-0174-z
- Bonino B, Murea M, Linville L. Uric acid in CKD: has the jury come to the verdict? J Nephrol. 2020;33(4):715-24. Availablefrom: https://doi.org/10.1007/s40620-020-00702-7
- Kamatani N, Fujimori S, Hieda S. An allopurinol-controlled, multicenter, randomized, open-label, parallel between-group, comparative study of febuxostat (TMX67), a non-purine-selective inhibitor of xanthine oxidase, in patients with hyperuricemia including those with gout in Japan: phase 2 exploratory clinical study. J Clin Rheumatol. 2011;17(4 Suppl 2):S44-9.
- Kidney Disease: Improving Global Outcomes (KDIGO). KDIGO 2012 Clinical Practice Guideline for the Evaluation and Management of Chronic Kidney Disease [Internet]. 2013 [cited 2024 Aug6]. Available from:https://kdigo.org/wp-content/uploads/2017/02/KDIGO_2012_CKD_GL.pdf
- Sonoda H, Takase O, Kato N, Kimura G. Uric acid levels predict future development of chronic kidney disease. Am J Nephrol. 2011;33(4):352-7. Available from: https://doi.org/10.1159/000326848
- Yamada T, Fukatsu M, Suzuki S, Wada T, Joh T. Elevated serum uric acid predicts chronic kidney disease. Am J Med Sci. 2011;342(6):461-6. Available from: https://doi.org/10.1097/maj.0b013e318218bd89
- Mwasongwe SE, Fülöp T, Katz R, Musani SK, Sims M, Correa A, et al. Relation of uric acid level to rapid kidney function decline and development of kidney disease: The Jackson Heart Study. J Clin Hypertens (Greenwich). 2018;20(4):775-83. Availablefrom: https://doi.org/10.1111/jch.13239
- Son YB, Yang JH, Kim MG, Jo SK, Cho WY, Oh SW. The effect of baseline serum uric acid on chronic kidney disease in normotensive, normoglycemic, and non-obese individuals: a health checkup cohort study. PLoS One. 2021;16(1):e0244106. https://doi.org/10.1371/journal.pone.0244106
- Toyama T, Furuichi K, Shimizu M, Hara A, Iwata Y, Sakai N, et al. Relationship between serum uric acid levels and chronic kidney disease in a Japanese cohort with normal or mildly reduced kidney function. PLoS One. 2015;10(9):e0137449. Availablefrom: https://doi.org/10.1371/journal.pone.0137449
- Iseki K, Ikemiya Y, Inoue T, Iseki C, Kinjo K, Takishita S. Significance of hyperuricemia as a risk factor for developing ESRD in a screened cohort. Am J Kidney Dis. 2004;44(4):642-50.
- Johnson RJ, Lozada LGS, Lanaspa MA, Piani F, Borghi C. Uric acid and chronic kidney disease: still more to do. Kidney Int Rep. 2023;8(2):229-39. Available from: https://doi.org/10.1016/j.ekir.2022.11.016
- Weiner DE, Tighiouart H, Elsayed EF, Griffith JL, Salem DN, Levey AS. Uric acid and incident kidney disease in the community. J Am Soc Nephrol. 2008;19(6):1204-11. Available from: https://doi.org/10.1681/asn.2007101075
- Prezelin-Reydit M, Speyer R, Saad N. Longitudinal uric acid has nonlinear association with kidney failure and mortality in chronic kidney disease. Sci Rep. 2023;13(1):17602.
- Yin Y, Zhou E, Wu J. Association between hyperuricemia and long-term mortality in patients with hypertension: results from the NHANES 2001-2018. Front Cardiovasc Med. 2024;11:1347917.
- Weis L, Metzger M, Haymann JP, Thervet E, Flamant M, Vrtovsnik F, et al. Renal function can improve at any stage of chronic kidney disease. PLoS One. 2013;8(12):e81835. Availablefrom: https://doi.org/10.1371/journal.pone.0081835
- National Kidney Foundation. K/DOQI clinical practice guidelines for chronic kidney disease: evaluation, classification, and stratification. Am J Kidney Dis. 2002;39(2 Suppl 1):S1-266.
- Inker LA, Astor BC, Fox CH, Isakova T, Lash JP, Peralta CA, et al. KDOQI US commentary on the 2012 KDIGO clinical practice guideline for the evaluation and management of CKD. Am J Kidney Dis. 2014;63(5):713-35. Available from: https://doi.org/10.1053/j.ajkd.2014.01.416
- Goicoechea M, de Vinuesa SG, Verdalles U, Ruiz-Caro C, Ampuero J, Rincón A, et al. Effect of allopurinol in chronic kidney disease progression and cardiovascular risk. Clin J Am Soc Nephrol. 2010;5(8):1388-93. Available from: https://doi.org/10.2215/cjn.01580210
- Zhang TJ, Zhang X, Xu EY, Wang ZR, Zhang ZH, Wang QY, Wang L, Wen YQ, Meng FH. A possible covalent xanthine oxidase inhibitor TS10: Inhibition mechanism, metabolites identification and PDPK assessment. Bioorg Chem. 2022 Nov;128:106064. Available from: https://doi.org/10.1016/j.bioorg.2022.106064
- Maruyama Y, Tanaka T, Tanabe K, et al. Effect of uric acid-lowering therapy on renal function in patients with chronic kidney disease: a systematic review and meta-analysis. Ren Replace Ther. 2021;7(1):15.