
More Information
Submitted: May 07, 2026 | Accepted: May 13, 2026 | Published: May 14, 2026
Citation: Sabi AK, Blatome LO, Dolaama B, Tsevi YM, Amede AD, Haroune-Traore J, et al. Acute Kidney Injury and Ad Hoc Consultancy Opinions of Nephrology Consultants in the Ivory Coast: Epidemiological, Diagnostic, and Prognostic Aspects. J Clini Nephrol. 2026; 10(5): 44-49. Available from:
https://dx.doi.org/10.29328/journal.jcn.1001175
DOI: 10.29328/journal.jcn.1001175
Copyright license: © 2026 Sabi AK, et al. This is an open access article distributed under the Creative Commons Attribution License, which permits unrestricted use, distribution, and reproduction in any medium, provided the original work is properly cited.
Keywords: Acute kidney injury; Expert opinion

Acute Kidney Injury and Ad Hoc Consultancy Opinions of Nephrology Consultants in the Ivory Coast: Epidemiological, Diagnostic, and Prognostic Aspects
Akomola Kossi Sabi1, Laune Odilon Blatome2,3* , Badomta Dolaama1, Yawovi Mawufemo Tsevi1, Amah Daniel Amede4, Jannat Haroune-Traore4, Eyram Yoan Makafui Amekoudi2, Monlet Cyr Guei3, Delphine Amélie Lagou3 and Kan Clément Ackoundou-N’guessan3
, Badomta Dolaama1, Yawovi Mawufemo Tsevi1, Amah Daniel Amede4, Jannat Haroune-Traore4, Eyram Yoan Makafui Amekoudi2, Monlet Cyr Guei3, Delphine Amélie Lagou3 and Kan Clément Ackoundou-N’guessan3
1Nephrology and Hemodialysis Department, Sylvanus Olympio University Hospital of Lomé, Togo
2Nephrology Department, Kara University Hospital, Togo
3Nephrology Department, Yopougon University Hospital; Félix Houphouët-Boigny University, Ivory Coast
4Nephrology-Internal Medicine D Department, Treicheville University Hospital; Department of Medicine and Medical Specialties, UFR of Medical Sciences, Félix Houphouët-Boigny University, Ivory Coast
*Corresponding author: Laune Odilon Blatome, Nephrology Department, Kara University Hospital, TOGO, Email: [email protected]
Context: Acute kidney injury is a serious and frequently encountered condition in hospital settings, with an increasing incidence. Given the increasing number of evidence reporting the benefits of specialized and early nephrology care, the Ad Hoc Consultancy Opinion regains a crucial interest in the nephrology care pathway. In the Ivory Coast, data concerning this activity are rare. The objective of this study was therefore to evaluate the Ad Hoc Consultancy Opinion impacts under our practice conditions.
Methods: Our study will focus on all patients of the CHU Treicheville without a history of kidney disease seen in the Ad Hoc Consultancy Opinion by the nephrology team of said center over the period from October 1, 2022, to March 31, 2023.
Results: The consultative nephrology service involved 106 patients with an average age of 45.1 +/- 21.1 years. The average delay for requesting the consultation was 2.6 +/- 2.5 days. Acute kidney injury was at stage 3 of the KDIGO classification in 73.6% (n = 78). Emergency hemodialysis accounted for 59.4% of the indications. The mortality was 22.6%, and the risk of death was associated with coma (p = 0.014), left heart failure (p = 0.009), ARDS (p = 0.035), the severity of AKI (p = 0.024), and the Ad Hoc Consultancy Opinion delay > 3 days (p = 0.010).
Conclusion: Our study adds weight to the claims that early specialized management of kidney disease affects the nephrological outcome and survival of patients.
Acute kidney injury (AKI) is a serious and frequently encountered condition in hospital settings, with an increasing incidence [1]. It is responsible for significant morbidity and mortality, including a four-fold increase in the risk of in-hospital mortality [1,2]. Given the growing evidence reporting the benefits of specialized and early nephrology care particularly regarding the slowing of disease progression, the reduction of hospitalization duration, and decreased mortality the Kidney Disease Improving Global Outcomes (KDIGO) organization established reference criteria for nephrology practice in 2012 [3-7]. As the health workforce represents the cornerstone of any healthcare system, the Ad Hoc Consultancy Opinion (AHCO) holds paramount importance within the nephrology care pathway, as it serves to fulfill a key objective: optimizing access to care. In the Ivory Coast, however, data on this activity remain scarce or altogether absent. The aim of this study was therefore to provide insights into AKI among patients evaluated through AHCO. The working hypothesis is that early management of kidney diseases improves patient survival and their renal prognosis.
Patients
We conducted an analytical cross-sectional study with prospective data collection on a consecutive cohort of patients treated for AKI between October 1, 2022 and March 31, 2023 at the Treichville University Hospital Center (CHU).
Methods
This was an exhaustive sampling, including patients without a history of kidney disease seen in AHCO and followed for AKI over the duration of hospitalization by the nephrology team of the said center. Data were collected using a standardized electronic form deployed on the KoBoToolbox platform, alongside the clinical hospitalization records. The database was cleaned and analyzed using R software (version 4.3.1).
The parameters studied included socio-demographic, anamnestic, diagnostic, therapeutic, and evolutionary data. Qualitative variables were presented according to their frequencies and proportions, and quantitative variables according to their means, standard deviations, medians, and interquartile ranges. For the comparison of proportions, the Chi-square and Fisher’s exact tests were used according to their validity conditions. To compare means and medians, normality of distribution was first assessed using the Shapiro-Wilk test, after which nonparametric tests (Kruskal-Wallis and Mann-Whitney) were applied. The significance threshold was set at p < 0.05.
Operational definition
Epidemiological data
During the study period, the nephrology department received 106 consultation requests for acute kidney injury, including 54 men, with a sex ratio of 1.04. The mean age of the patients was 45.1 ± 21.1 years, with a range of 2 to 82 years. The most affected age group was 45–54 years (24.5%) (Figure 1).
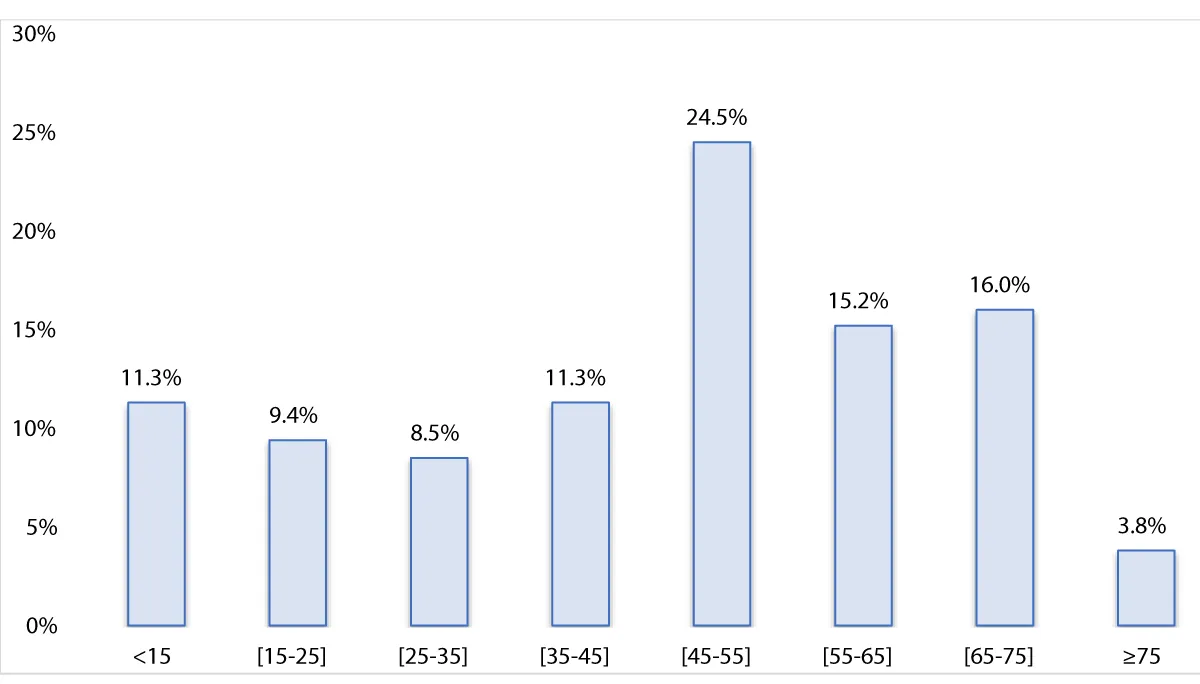
Figure 1: Distribution of patients by age group in years
The mean time to AHCO after identification of nephrological abnormalities or symptoms was 2.6 ± 2.5 days. The departments that most frequently requested nephrology consultations were infectious diseases (24.5%) and medical emergencies (20.8%) (Figure 2).
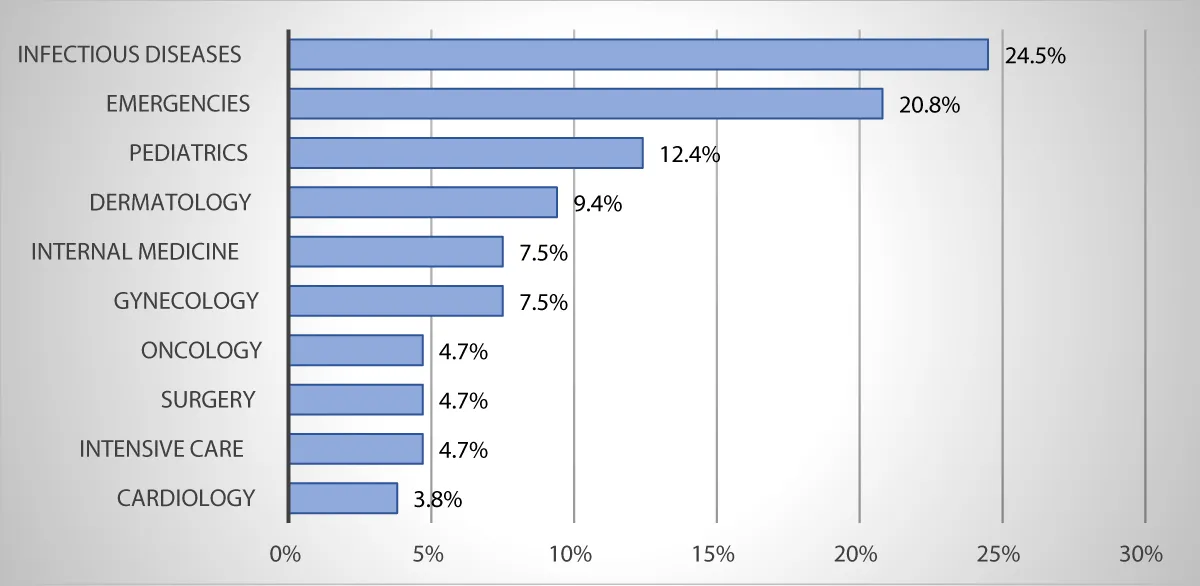
Figure 2: Distribution of patients by inpatient department.
Clinical and paraclinical data
The reason for consultation request was renal function impairment in 100% of cases. Regarding medical history, there were 23 cases of arterial hypertension (21.7%), 18 cases of diabetes mellitus (17.0%), 15 cases of human immunodeficiency virus (HIV) infection (14.2%), and one case of scleroderma (0.9%). The main findings on clinical examination were conjunctival pallor (69.8%), fever (58.5%), and oligoanuria (53.8%).
On biological assessment, anemia was present in 86.8% (n=92) of cases, with a mean hemoglobin level of 8.6 ± 2.7 g/dL (range: 3.0 to 13.8 g/dL). The mean serum creatinine was 98 ± 88.2 mg/L (range: 16 to 438 mg/L) and the mean serum urea was 1.8 ± 1.1 g/L (range: 0.5 to 4.9 g/L). Blood ionogram analysis revealed 83 cases of hyponatremia and 33 cases of hyperkalemia. The infectious workup identified 37 cases of malaria, 5 cases of urinary tract infection, and 5 cases of amicrobial leukocyturia out of 13 urine cytobacteriological examination (UCBE) samples performed, as well as 4 cases of streptococcal infection (ASLO positive) out of 8 samples tested.
Diagnostic and prognostic data
AKI was at stage 3 of the KDIGO classification in 73.6% of cases (n = 78). Based on the clinical circumstances and the pathophysiological factors identified, renal involvement was parenchymal in 67.0% of cases (Table 1). Regarding toxic or drug-related causes, polypharmacy (combination of antimalarial agents and ciprofloxacin) was identified in one case, and phytotherapy in 3 cases.
| Table 1: Summary of the lesional and etiological diagnosis | |||
| Lesion diagnosis | Etiological diagnosis | Workforce | Percentage |
| Pre-renal | 20 | 18,9% | |
| DEC | 11 | 10,5% | |
| Low cardiac output | 08 | 07,5% | |
| Hemorrhagic fibroid | 01 | 00,9% | |
| Parenchymal | 71 | 67,0% | |
| ATN | 57 | 53,7% | |
| Sepsis | 52 | 49,0% | |
| Toxic | 04 | 03,8% | |
| Hemorrhagic | 01 | 00,9% | |
| AGN | 05 | 04,7% | |
| Post Streptococcal | 04 | 03,8% | |
| Undetermined | 01 | 00,9% | |
| AVN | 05 | 04,7% | |
| Pregnancy | 03 | 02,9% | |
| CRS | 01 | 00,9% | |
| MNAS | 01 | 00,9% | |
| AIN | 04 | 03,8% | |
| Infectious pyelonephritis | 02 | 01,9% | |
| Sepsis | 02 | 01,9% | |
| Postpenal | 15 | 14,2% | |
| Enlarged prostate | 10 | 09,5% | |
| Urolithiasis | 02 | 01,9% | |
| Uterine tumor | 02 | 01,9% | |
| Bladder tumor | 01 | 00,9% | |
| DEC: Extracellular Dehydration; CRS: Scleroderma Renal Crisis; ATN: Acute Tubular Necrosis; AGN: Acute Glomerulonephritis; AIN: Acute Interstitial Nephritis; AVN: Acute Vasculitis Nephropathy; MNAS: Malignant Nephroangiosclerosis. |
|||
Emergency dialysis was indicated in 32 patients and initiated in 19, representing 59.4% of indications. The indications for emergency dialysis were uremic encephalopathy (22.6%), severe uremia (17.9%), and anuria lasting more than 48 hours (17.0%), hyperkalemia (4.7%), and acute pulmonary edema (APE) (4.7%).
Clinical evolution was favorable in 52.8% of cases, with complete recovery in 28.3% and partial recovery in 24.5%. The dialysis weaning rate was 63.2% among dialyzed patients (n = 12), and mortality was 22.6% during the study period. The risk of death was significantly associated with coma (p = 0.014), left heart failure (p = 0.009), acute respiratory distress syndrome (ARDS) (p = 0.035), severity of AKI (p = 0.024), and delay in seeking nephrology consultation (p = 0.010) (Table 2).
| Table 2: Factors associated with the risk of death | ||||
| Variables | N | Deceased, n (%) | Alive, n (%) | p - value |
| Socio-demographics | ||||
| Gender | 106 | 0,6 | ||
| Female | 13 (54,2%) | 39 (47,6%) | ||
| Male | 11 (45,8%) | 43 (52,4%) | ||
| Age | 106 | 0,8 | ||
| < 60 years | 16 (66,7%) | 57 (69,5%) | ||
| ≥ 60 years old | 08 (33,3%) | 25 (30,5%) | ||
| Comorbidities | ||||
| Diabetes | 106 | 04 (16,7%) | 14 (17,1%) | > 0,9 |
| HIV | 53 | 06 (46,2%) | 09 (22,5%) | 0,2 |
| Clinical | ||||
| Fever | 106 | 14 (58,3%) | 55 (67,1%) | 0,4 |
| Coma | 106 | 14 (58,3%) | 23 (28,0%) | 0,014 |
| Oligo-anurie | 106 | 11 (45,8%) | 46 (56,1%) | 0,4 |
| Left heart failure | 106 | 04 (16,7%) | 01 (01,2%) | 0,009 |
| Right heart failure | 106 | 00 (00,0%) | 02 (02,4%) | > 0,9 |
| ARDS | 106 | 08 (33,3%) | 11 (13,4%) | 0,035 |
| Paraclinic | ||||
| Natremia | 106 | 0,2 | ||
| Normal | 07 (29,2%) | 14 (17,1%) | ||
| Severe hyponatremia | 02 (08,3%) | 05 (06,1%) | ||
| Mild to moderate hyponatremia | 14 (58,3%) | 62 (75,6%) | ||
| Hypernatremia | 01 (04,2%) | 01 (01,2%) | ||
| Kaliemia | 106 | 0,7 | ||
| Normal | 14 (58,3%) | 46 (56,1%) | ||
| Hypokalemia | 02 (08,3%) | 11 (13,4%) | ||
| Mild to moderate hyperkalemia | 08 (33,4%) | 21 (25,6%) | ||
| Severe hyperkalémia | 00 (00,0%) | 04 (04,9%) | ||
| Severe anemia | 106 | 09 (37,5%) | 40 (48,8%) | 0,3 |
| Other | ||||
| Time limit for requesting the opinion | 106 | 0,010 | ||
| ≤ 24 hours | 12 (50,0%) | 44 (53,7%) | ||
| [1 - 3] days | 03 (12,5%) | 28 (34,1%) | ||
| > 3 days | 09 (37,5%) | 10 (12,2%) | ||
| Severity of the IRA | 106 | 0,024 | ||
| Stage 1 | 00 (00,0%) | 17 (20,7%) | ||
| Stage 2 | 05 (20,8%) | 06 (07,3%) | ||
| Stage 3 | 19 (79,2%) | 59 (72,0%) | ||
Epidemiological data
In our study, the patients were predominantly young adults. This is consistent with the findings of Failal, et al. in Morocco (2020), Konan, et al. in Ivory Coast (2021), and Samake, et al. in Mali (2022) [12–14]. However, these results diverge from data reported in developed countries, where the mean age was generally above 60 years [15,16]. This discrepancy may be explained by demographic characteristics, notably the relatively young age structure of African populations compared to the increasingly aging populations of developed countries.
Male predominance has been reported in numerous African and Western studies, consistent with the findings of the present study [12,14,15]. However, in Ivory Coast, Yao, et al. (2017) and Guei, et al. (2019) reported female predominance in their studies conducted among HIV-infected patients [17,18]. This finding may be attributed to the higher prevalence of HIV infection among women in this population [19].
Renal function impairment was the sole indication for AHCO in all cases. Consistent with studies on initial and follow-up nephrology consultations conducted in Senegal, Australia, and Great Britain, renal function impairment represented the primary reason for referral to nephrology expertise [20–22]. It is worth noting, however, that in our region, the indications for nephrology referral are considerably less varied compared to those reported in developed countries. Indeed, the diagnosis of kidney disease typically arises in two distinct clinical situations: on the one hand, during the follow-up of patients at risk, such as those with hypertension, diabetes mellitus, or autoimmune disease; and on the other hand, in the presence of clinical signs suggestive of kidney injury. In both situations, the need for referral to specialized nephrology care should be systematically assessed in accordance with the recommendations of learned societies [10,23].
Diagnostic and prognostic data
The majority of patients (73.6%) presented at stage 3 of the KDIGO classification, with a considerable proportion requiring emergency dialysis (30.2%). These findings are consistent with those reported by Guei ,et al. (61.6% at stage 3), and suggest late diagnosis and/or delayed management of patients [18]. Favre, in a study on the timing of nephrology consultation requests, recommends a referral delay of less than 2 hours to avoid missing a vital emergency; yet in the present series, the mean time to specialist consultation request was 2.6 ± 2.5 days [24]. These data highlight a significant weakness in our healthcare system, namely the delayed response of healthcare staff to clinical deterioration.
Complete recovery was recorded in 28.3% of cases and partial recovery in 24.5%. Lengani et al. reported higher rates in Burkina Faso, with complete recovery in 41.3% and partial recovery in 36.4% of cases [25]. According to the literature, approximately 63% of patients regained their baseline renal function following an episode of AKI, with a lower proportion observed among patients with pre-existing chronic kidney disease (CKD) [26]. The dialysis withdrawal rate of 63.2% observed in the present study is consistent with data from the literature, which reports rates ranging from 40% to 70% [27–29].
The mortality rate in the present study was 22.6%. With an estimated 1.7 million deaths attributed to acute kidney disease annually worldwide, the close association between AKI and mortality is well established [30].
In numerous studies on AKI, the risk of mortality has been correlated with the severity of renal impairment and associated vital organ failures [26,28]. The findings of the present study are consistent with these observations, identifying a significantly increased risk of death associated not only with coma (p = 0.014), left heart failure (p = 0.009), and acute respiratory distress syndrome (ARDS) (p = 0.035), but also with the severity of AKI (p = 0.024) and a delay in requesting nephrology consultation exceeding 3 days (p = 0.010). The latter finding further supports the growing body of evidence suggesting that early specialized nephrology care is associated with a reduction in mortality [6,31–33].
Our working hypothesis is confirmed with a risk of death associated with the severity of kidney damage and a delay in requesting consultation of more than 3 days. AKI in our countries predominantly affects young adult males, with infectious etiologies representing the leading cause. Despite the advent of renal replacement therapy, which has substantially transformed the management of severe renal failure, mortality rates remain unacceptably high, largely attributable to delayed diagnosis and referral to specialized care. These findings highlight the critical importance of a comprehensive and coordinated approach, encompassing public awareness campaigns, improved access to nephrology care, and the continuous training of healthcare personnel on the clinical benefits of early specialized nephrology intervention. Further prospective multicenter studies are warranted to better characterize the epidemiological and clinical profile of AKI in our countries and to inform evidence-based nephrology care policies.
- Kahindo CK, Mukuku O, Wembonyama SO, Tsongo ZK. Prevalence and factors associated with acute kidney injury in adults in sub-Saharan Africa: a review of the current literature. Int J Nephrol. 2022;2022:5621665. Available from: https://doi.org/10.1155/2022/5621665
- Sawhney S, Marks A, Fluck N, Levin A, Prescott G, Black C. Intermediate and long-term outcomes of survivors of acute kidney injury episodes: a large population-based cohort study. Am J Kidney Dis. 2017;69(1):18-28. Available from: https://doi.org/10.1053/j.ajkd.2016.05.018
- Smart NA, Dieberg G, Ladhani M, Titus T. Early referral to specialist nephrology services for preventing the progression to end-stage kidney disease. Cochrane Database of Systematic Reviews. 2014;18(6): CD007333. Available from: https://doi.org/10.1002/14651858.cd007333.pub2
- Hommel K, Madsen M, Kamper AL. The importance of early referral for the treatment of chronic kidney disease: a Danish nationwide cohort study. BMC Nephrology. 2012;13:108. Available from: https://doi.org/10.1186/1471-2369-13-108
- Levin A, Stevens PE, Bilous RW, et al. Kidney disease: Improving global outcomes (KDIGO) CKD work group. KDIGO 2012 clinical practice guideline for the evaluation and management of chronic kidney disease. Kidney Int Suppl. 2013. Available from: https://doi.org/10.1038/kisup.2012.73.
- Milkowski A, Prystacki T, Marcinkowski W, Dryl-Rydzynska T, Zawierucha J, Malyszko JS, et al. Lack or inadequacy of predialysis nephrology care worsens outcomes in dialysis patients – call to action. Renal Failure. 2022;44(1):946-57. Available from: https://doi.org/10.1080/0886022x.2022.2081178
- Ghimire A, Ye F, Hemmelgarn B, Zaidi D, Jindal KK, Tonelli MA, et al. Trends in nephrology referral patterns for patients with chronic kidney disease: Retrospective cohort study. PLoS ONE. 2022;17(8): e0272689. Available from: https://doi.org/10.1371/journal.pone.0272689
- Acute Renal Failure - Anuria Item 348 - [Manual of Nephrology 10th Edition] Chapter 14 [Internet]. 10th EDITION 2024.
- Babitt JL, Berns JS, Bozkurt B, Cheung Khedairy RS, Cuevas Y, Effa EE, et al. KDIGO Anemia Guideline Executive Summary. Kidney International. 2026;109:44-56. Available from: https://doi.org/10.1016/j.kint.2025.06.005
- Stevens PE, Ahmed SB, Carrero JJ, Foster B, Francis A, Hall RK, et al. KDIGO 2024 Clinical Practice Guideline for the Evaluation and Management of Chronic Kidney Disease. Kidney International. 2024;105(4S):S117-S314. Available from: https://doi.org/10.1016/j.kint.2023.10.018.
- Prescott H, Antonelli M, Alhazzani W, Moller MH, Alshamsi F, Azevedo L, et al. Surviving Sepsis Campaign: International Guidelines for Management of Sepsis and Septic Shock 2026. Crit Care Med. 2026 ;54(4):725-812. Available from: https://doi.org/10.1097/ccm.0000000000007075
- Konan SD, Diopoh SP, Guei MC, Sanogo S, Aka JA, Ouattara A, Yao KH. Acute Renal Failure and Hemodialysis: Clinical, Biological and Evolutionary Aspects at the Department of Nephrology-Internal Medicine D of the Treichville University Hospital. Health Sci. Dis: 2021;22(10):7-14. Available from: https://doi.org/10.1111/nep.13064
- Samaké M, Sy S, Fofana A, Yattara H, Coulibaly S, Diallo D, et al. Epidemiological and clinical profile of patients undergoing primary nephrological consultation at Fousseyni DAOU Hospital in Kayes, Mali. Open Journal of Nephrology. 2022;12(1):142-53. Available from: https://doi.org/10.4236/ojneph.2022.121014
- Failal I, Ezzaki S, Mtioui N, Elkhayat S.S, Zamed M, Medkouri G, et al. Acute renal failure: epidemiological, etiology, therapeutic and progressive profile. Nephrol ther. 2020; 16(5):326.
- Montgomerie C, Spaak J, Evans M, Jacobson S.H. Acute Kidney Injury: Clinical Characteristics and Short-Term Outcomes in 1,519 Patients. Kidney Dis. 2023;9:39-48. Available from: https://doi.org/10.1159/000527299.
- Wu Y, Luo L, Sun X, Ye X, Ren Y, Zhang W, et al. A closer look at severe acute kidney injury: risk factors and treatment outcomes with antibody-1/-L1 from a retrospective study. PairJ. 2025; 13:E19886. Available from: https://doi.org/10.7717/PeerJ.19886.
- Yao KH, Tanon AK, Lagou AD, Konan SD, Diopoh SP, Meite F. Comparative study of community-based acute kidney failure in HIV-positive and HIV-negative subjects: experience of an internal medicine department in Abidjan (Ivory Coast). Nephrol ther. 2017. Available from: https://doi.org/10.1016/J.Nephro.2016.10.003.
- Guei M.C, Sidibé M, Wognin A, Konan S.D, Choho M.C, Yao KH, et al. Outcome of acute renal failure in subjects with HIV living in Abidjan, Ivory Coast over the period 1st January 2014 to 31st December 2017. PAMJ. 2019;34:2. Available from: https://doi.org/10.11604/pamj.2019.34.2.20016.
- Kouame KB. Update of the Ivory Coast. The second all-network dHTS meeting. 2024; Durban.
- Faye MO, Ait AI, Lemrabott AT, Faye M, Cisse MM, Fall K, et al. (2018) Clinical and Paraclinical Profile of Patients in First Nephrology Consultation at the Aristide Le Dantec University Hospital Center (ALD-UHC) About 542 Cases. J Nephrol Kidney Dis. 2020;1(1):101. Available from: https://doi.org/10.15744/2767-9225.1.101
- Burke MT, Kapojos J, Sammartino C, Gray NA. Kidney Disease Health Literacy among New Patients Referred to a Nephrology Outpatient Clinic. Internal Medicine Journal. 2014;44:1080-6. Available from: https://doi.org/10.1111/imj.12519
- Prévot J, Bayat-Makoei S, Vigneau C. Reasons for first consultation in nephrology in health area 5 of Brittany during the year 2014. Nephrol ther 2017;13(2):67-75. Available from: https://doi.org/10.1016/j.nephro.2016.09.003
- Haute Autorité de santé (HAS) (2021) Guide to the care pathway. Chronic kidney disease in adults. Available from: https://www.has-sante.fr/upload/docs/application/pdf/202109/guide__mrc.pdf
- Favre N, Burnier M, Kissling S. When to call the nephrologist in the emergency room? Rev Med Switzerland. 2016;12:398-403.
- Lengani A, Kargougou D, Fogazzi GB, Laville M. Acute kidney injury in Burkina Faso. Nephrol Ther. 2010; 6(1):28-34. Available from: https://doi.org/10.1016/j.nephro.2009.07.013
- Aniort J, Heng A, Deteix P, Souweine B, Lautrette A. Epidemiology of acute renal failure. Nephrol Ther. 2019;15:63-9. Available from: https://doi.org/10.1016/j.nephro.2018.11.002
- Diawara MS, Kane Y, Cisse MM, Lemrabott AT, Faye M, Bop MC et al. Hemodialysis in Emergency Situations: A Study of 107 Cases at the Hemodialysis Center of the CHR of Thiès (Senegal). Health Sci. Dis. 2020;21(3):48-52. Available from:https://doi.org/10.28933/gjun-2019-12-2205
- Ilboudo CS, Doro H, Guibla I, Belem F, Konate S, Semdé A, et al. Prognosis of Emergency Hemodialysis Patients in the Nephrology and Dialysis Department of the Souro Sanou University Hospital Center (Bobo Dioulasso). Health Sci. 2021;6:11-4. Available from: https://doi.org/10.5281/hsd.v22i6.2806
- Chijioke A, Makusidi AM, Rafiu MO. Factors influencing hemodialysis and outcome in severe acute renal failure from Ilorin, Nigeria. Saudi J Kidney Dis Transpl 2012;23:391-6. Available from: https://pubmed.ncbi.nlm.nih.gov/22382247/
- Mehta RL, Cerda J, Burdmann EA, et al. International Society of Nephrology’s 0by25 initiative for acute kidney injury (zero preventable deaths by 2025): a human rights case for nephrology. Lancet. 2015;385:2616-43. Available from: https://doi.org/10.1016/s0140-6736(15)60126-x
- Singh K, Waikar SS, Samal L. Assessing the Feasibility of KDIGO CKD Reference Recommendations. BMC Nephrol. 2017;18(1):223.
- Hommel K, Madsen M, Kamper AL. The importance of early referral for the treatment of chronic kidney disease: a Danish nationwide cohort study. BMC Nephrology. 2012;13:1. Available from: https://doi.org/10.1186/s12882-017-0646-y
- Smart NA, Dieberg G, Ladhani M, Titus T. Early referral to specialist nephrology services for preventing the progression to end-stage kidney disease. Cochrane Database of Systematic Reviews. 2014; 18(6):CD007333. Available from: https://doi.org/10.1002/14651858.cd007333.pub2