
More Information
Submitted: April 29, 2024 | Approved: May 09, 2024 | Published: May 10, 2024
How to cite this article: Mourabiti L, Allata Y, El Bardai G, Chouhani BA, Kabbali N, et al. Renal Lymphangiectasia: A Diagnostic and Therapeutic Challenge. J Clini Nephrol. 2024; 8: 055-059.
DOI: 10.29328/journal.jcn.1001127
Copyright License: © 2024 Mourabiti L, et al. This is an open access article distributed under the Creative Commons Attribution License, which permits unrestricted use, distribution, and reproduction in any medium, provided the original work is properly cited.
Keywords: Renal lymphangiectasia; Cystic infiltration; Diagnostic approach; Therapeutic strategies; Personalized management

Renal Lymphangiectasia: A Diagnostic and Therapeutic Challenge
Mourabiti L*, Allata Y1,2, El Bardai G1,2, Chouhani BA1,2, Kabbali N1,2, Sqalli Houssaini T1-3, Bouabdallah Y2,4,5, Khattala K2,4, Alaoui O2,4, Boubou M2,6, Hida M2,7,8 and Souilmi FZ2,8
1Department of Nephrology, Dialysis Renal Transplantation at the Hassan II University Hospital Center of Fez, Morocco
2Laboratory of Epidemiology and Research in Health Sciences, Faculty of Medicine, Pharmacy, and Dental Medicine, Sidi Mohamed Ben Abdellah University, Fez, Morocco
3Head of the Department of Nephrology, Dialysis Renal Transplantation at the Hassan II University Hospital Center of Fez, Morocco
4Department of Pediatric Surgery at the Hassan II University Hospital Center of Fez, Morocco
5Head of the Department of Pediatric Surgery at the Hassan II University Hospital Center of Fez, Morocco
6Department of Radiology at the Hassan II University Hospital Center of Fez, Morocco
7Head of the Department of Pediatrics at the Hassan II University Hospital Center of Fez, Morocco
8Department of Pediatrics at the Hassan II University Hospital Center of Fez, Morocco
*Address for Correspondence: Mourabiti L, Department of Nephrology, Dialysis Renal Transplantation at the Hassan II University Hospital Center of Fez, Morocco, Email: [email protected]
Renal lymphangiectasia, a rare lymphatic disorder, manifests as cystic infiltration in the perirenal and para-pyelic space due to lymphatic drainage defects. Diagnosis hinges on imaging modalities like ultrasound, CT, and MRI. However, lack of awareness can lead to confusion with other renal cystic pathologies. Here, we present a case of renal lymphangiectasia in a child, detailing diagnostic and therapeutic strategies. The patient, a 2-year-old and 2-month-old girl from a consanguineous marriage, presented with persistent abdominal distension. Clinical examination revealed growth retardation and normal blood pressure but abdominal distension with dullness. Lab investigations indicated acute renal failure with non-nephrotic proteinuria. Radiologically, renal lymphangiectasia was confirmed by ultrasound showing microcysts and perirenal cystic lesions with ascites, corroborated by MRI and CT scans. Treatment involved nephroprotective therapy and diuretics for ascites. Surgical intervention was necessitated due to cyst size and compressive nature, involving iterative punctures, marsupialization, and percutaneous drainage. Postoperatively, recurrent ascites temporarily worsened renal function but returned to baseline afterward. renal lymphangiectasia necessitates careful management due to its potential to progress to chronic renal failure. The prognosis depends on factors like initial proteinuria severity, treatment response, and complication management. Personalized approaches are pivotal in its diagnosis and management.
Renal lymphangiectasia is a rare lymphatic disorder scarcely described in medical literature, accounting for approximately 1% of all lymphangiomas [1]. marked by cystic infiltration into the perirenal and parapelvic space, stemming from a drainage anomaly within the lymphatic pathways. Diagnosis predominantly hinges on ultrasound, Computed Tomography (CT), and particularly Magnetic Resonance Imaging (MRI). Nonetheless, insufficient recognition of this condition may occasionally result in misidentification, particularly with other cystic renal ailments such as polycystic kidney disease. In this report, we present a case study involving a child diagnosed with renal lymphangiectasia, outlining both the diagnostic and therapeutic strategies employed.
A 2-year and 2-month-old girl, born from a consanguineous marriage, was admitted to the hospital for investigation of persistent abdominal distension lasting over a year. Family and perinatal histories were unremarkable, but clinical examination indicated delayed growth in stature and weight. Blood pressure fell within normal ranges according to reference curves, while abdominal examination revealed distension with shifting dullness. Biologically, acute renal failure was observed alongside non-nephrotic proteinuria. The diagnosis of renal lymphangiectasia was confirmed based on radiological findings: abdominal ultrasound depicted intracortical microcysts and a cluster of delicate-walled perirenal cystic lesions with anechoic content (Figure 1).
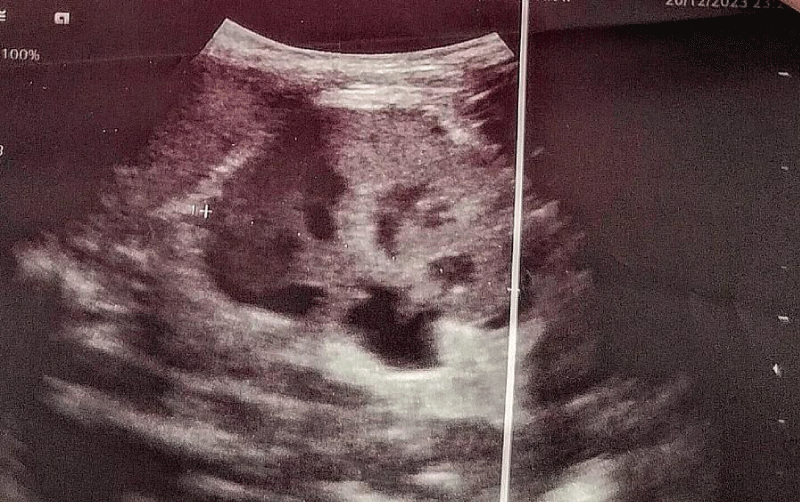
Figure 1: Presence of intracortical microcysts and a crown of contiguous perirenal cystic lesions, with thin walls, and anechoic content.
CT scans unveiled multiple bilateral intracortical renal cysts, coalescing and distorting kidney contours, remaining unaltered after contrast. Some cysts had ruptured into the perirenal area, leading to true bilateral perirenal collections with significant intra-peritoneal fluid effusion (Figure 2). MRI revealed numerous contiguous cortical micro cysts displaying T2 hyperintensity and T1 hypointensity, arranged in a bilateral perirenal cluster (Figures 3,4). These cysts exhibited thin walls enhanced after contrast, accompanied by a substantial amount of encapsulating ascites. Additionally, the liver appeared normal in size, with regular contours and homogeneous signals. Regarding treatment, the patient received nephroprotective therapy and diuretics. Due to the large size, bilaterality, and compressive nature of the cysts, surgical intervention was performed. This involved iterative drainage attempts, which proved futile, necessitating marsupialization with rupture and coagulation of the cysts, along with the placement of a percutaneous drain (Figure 5). Post-operative follow-up showed periods of remission and recurrence of ascites, resulting in temporary exacerbation of renal function and subsequent return to baseline renal function outside of the episode, with moderate renal insufficiency.

Figure 2: Abdominal CT scan in axial (a) and coronal (b) sections after contrast injection: multiple perirenal and parapelvic cysts with hypodense thin walls.
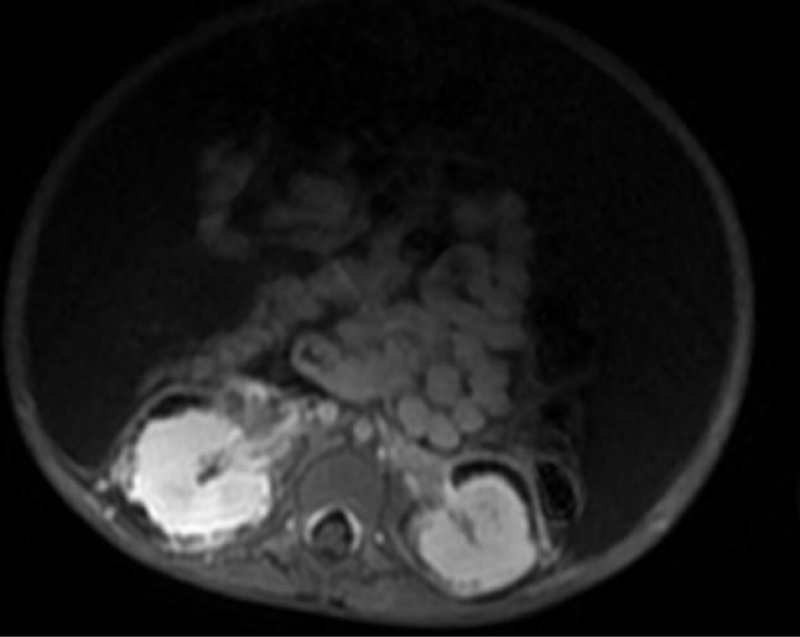
Figure 3: Axial section showing a bilateral perirenal fluid collection, compartmentalized, presenting as T1 hypointensity on MRI.
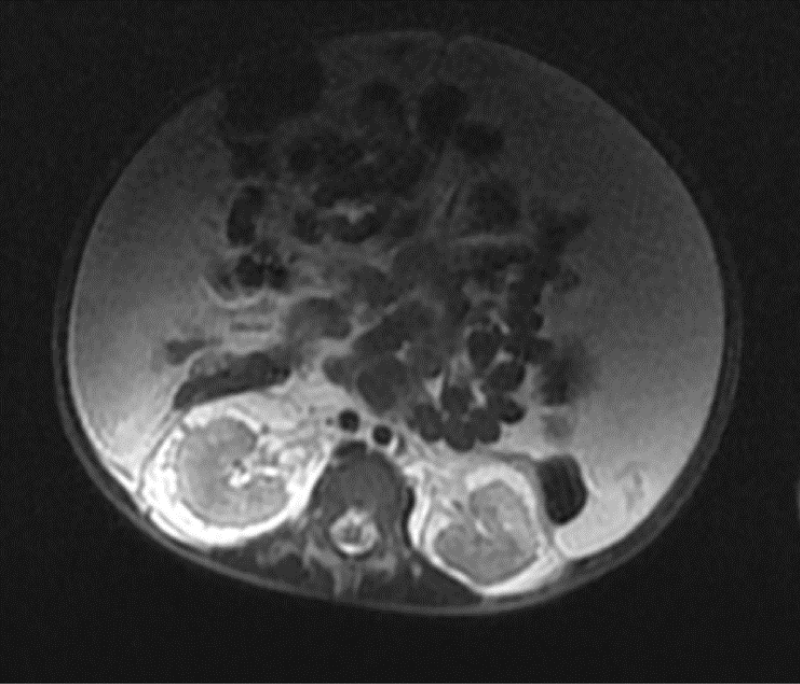
Figure 4: Axial section showing the presence of several bilateral cortical cysts which are in T2 hyperintensity on MRI.
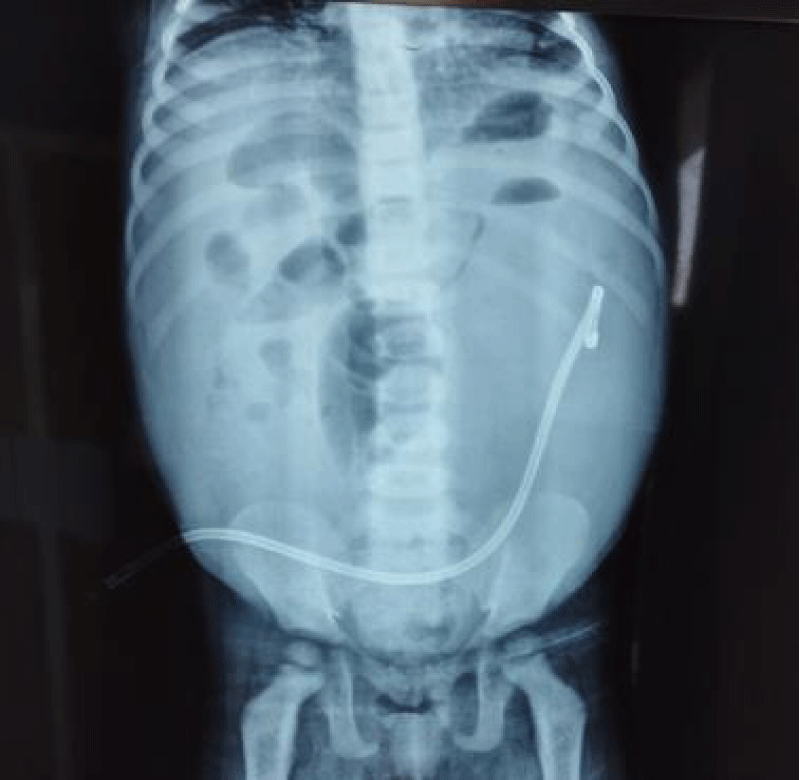
Figure 5: Ascites drainage by the insertion of a pigtail drain into the peritoneal cavity.
Renal lymphangiectasia is a rare benign lymphatic disorder, constituting approximately 1% of all lymphangiomas [1]. It can manifest in individuals of both sexes, spanning from children to adults, and may present unilaterally or bilaterally.
The precise pathophysiology remains elusive; however, it is postulated that the lymphatic drainage of the kidney, renal capsule, and perirenal tissues intercommunicate via several major lymphatic trunks within the renal sinus. These lymphatics typically drain toward retroperitoneal nodes, such as the para-aortic, para-caval, and inter-aorto-caval lymph nodes. In renal lymphangiectasia, whether unilateral or bilateral, a defect in the drainage of the lymphatic trunks within the renal sinus is presumed [2]. Embryonic lymphatic vessel development arises from the differentiation of venous endothelial cells into lymphatic endothelial cells, expressing LYVE-1 under the influence of various transcription factors, including PROX1, SOX18, and COUPTF2. These cells subsequently migrate and proliferate in the adjacent mesenchyme, forming primary lymphatic sacs, which, through expansion, give rise to the primitive arborescent lymphatic vascularization, regulated by the VEGF-C/VEGFR-3 signaling pathway and angiopoietin-1 [3], Several genes, such as CCBE1, ADAMTS3, FOXC2, NRP2, and GATA2, have been implicated in lymphatic channel and valve formation. Dysregulation of these genes may lead to increased lymphangiogenesis and cystic lymphatic malformation (CLM) formation. Some CLMs have been associated with activating somatic mutations of the PIK3CA gene [4], encoding the catalytic subunit of the PI3K protein kinase, resulting in aberrant activation of the PI3K/AKT/mTOR signaling pathway involved in angiogenesis, lymphangiogenesis, cell growth, and metabolism [5].
Clinical presentations of renal lymphangiectasia vary, with many cases being asymptomatic. Symptomatic instances may manifest as abdominal distension, back pain, hematuria, or limb edema. Severe cases may result in renal failure. In pediatric patients, a palpable abdominal mass is a common presentation. Blood pressure may be normal or elevated, with renal function typically remaining normal [6].
According to a literature review by Jorge Mejía Restrepo, et al. [7], renal lymphangiectasia exhibits two radiological manifestations. The first involves a cystic lesion within the renal sinus, presenting as small peripelvic cysts originating from the renal sinus or a large single parapelvic cyst originating from the medial renal parenchymal tissue. The second manifestation comprises lobular perirenal fluid with multiple septations and cysts within the renal sinus.
In ultrasound imaging, the cysts appear anechoic, often accompanied by a posterior shadow cone. Additional findings may include cortical hyperechogenicity or corticomedullary differentiation, indicative of interstitial edema secondary to intrarenal lymphatic drainage defects [8]. CT imaging typically depicts multicompartmental cysts with fluid density, which do not enhance after contrast injection. In MRI, cystic lesions appear hypointense in T1-weighted images and hyperintense in T2-weighted images. Occasionally, there may be a reversal of corticomedullary intensity in T2-weighted sequences, with the cortex appearing hyperintense and the medulla hypointense [9], attributed to density changes due to lymphatic obstruction-induced interstitial edema. The characteristic imaging appearance alone may suffice for diagnosing renal lymphangiectasia. In cases of uncertainty, an echo- or CT-guided cyst puncture may be performed, yielding fluid with a yellowish macroscopic appearance, rich in lymphocytes, and devoid of red blood cells [10].
Differential diagnoses encompass Autosomal Dominant Polycystic Kidney Disease (ADPKD), hydronephrosis, urinoma, renal lymphoma, and nephroblastoma. Arguments against ADPKD diagnosis include the absence of familial history, normal kidney size, and extraparenchymal localization of renal cysts.
Renal lymphoma typically presents as a perirenal lesion with tissue density on CT, enveloping the kidney, often confirmed as vascular by contrast enhancement. Exclusive renal involvement is observed in less than 10% of cases.
Urinomas, or urinary collections, frequently occur post-renal trauma or due to obstruction at the pyeloureteral junction, presenting as localized or diffuse cystic peritoneal masses on imaging.
Nephroblastomatosis, a malignant renal tumor arising from embryonic blastema, is characterized by diffuse renal enlargement with a hypoechoic appearance on ultrasound and soft tissue lesions with slight enhancement on CT scans, interspersed with normally enhanced adjacent renal parenchyma.
Complications of renal lymphangiectasia include hypertension resulting from renin-angiotensin system activation, dilation of peri-, centro-renal, and retroperitoneal lymphatics, potentially leading to compression of renal parenchyma and excretory pathways, resulting in hydronephrosis and subsequent renal failure. Other reported complications comprise hemorrhage and cystic infection [11].
Treatment selection for renal lymphangiectasia depends on clinical manifestations, with asymptomatic lesions requiring no specific intervention but necessitating periodic monitoring. Hypertension, ascites, and pain can be managed with antihypertensives, diuretics, and analgesics, respectively [12].
Percutaneous drainage of collections, with or without sclerosing agent injection, is warranted for less severe symptomatic cases and those with pain due to collection compression, although recurrence risk is elevated in particularly large lesions with multiple septations [13].
Percutaneous drainage with sclerotherapy is a safe and effective technique [14], often requiring multiple sessions due to disease complexity and recurrence rates [15]. Reported cases utilizing percutaneous drainage with sclerotherapy have demonstrated successful outcomes, with some utilizing doxycycline or povidone-iodine sclerotherapy approaches [16].
Marsupialization may be considered when a connection is established with the peritoneal cavity [17], especially for peripherally located cysts [18], although this procedure is not universally favored due to increased intraoperative bleeding and nephrectomy risks.
Nephrectomy serves as a therapeutic option following failed previous treatments or in cases of uncontrollable infection, bleeding, or suspected neoplastic changes. The preference or ultimate success of one therapeutic modality over another remains challenging to ascertain due to unique or limited case reports, precluding definitive conclusions regarding efficacy.
mTOR inhibitors have demonstrated efficacy in treating intestinal lymphangiectasia [19] and could potentially benefit intrarenal lymphangiectasia by inhibiting lymphangiogenesis [20]. However, no consensus currently exists regarding dosage and treatment duration. rapamycin is typically administered orally, with dosage adjustments guided by regular monitoring to achieve optimal concentrations.
While the literature predominantly focuses on clinical presentations, diagnostic modalities, and treatment options for renal lymphangiectasia, limited information is available regarding its long-term progression or contribution to chronic renal failure. Given the rarity of this condition, the exact rate of chronic renal failure attributable to renal lymphangiectasias remains poorly established. Prognosis hinges on various factors, including initial proteinuria severity, treatment response, and timely management of complications, significantly impacting patients’ quality of life and long-term survival prospects. Early diagnosis and appropriate management are crucial in reducing the risk of progression to chronic renal failure and improving overall survival rates.
Renal lymphangiectasia is a complex condition requiring meticulous management, which can progress to chronic renal failure in some cases. Surgical treatment options such as marsupialization or percutaneous drainage with sclerotherapy may be considered for symptomatic cases. mTOR inhibitors, although not commercially available in Morocco, have shown effectiveness in treating renal lymphangiectasia. The prognosis of lymphangiectasia is closely related to several key factors, including the initial severity of proteinuria, treatment response, and effective management of potential complications. This condition underscores the importance of a personalized approach in diagnosis and management.
- Hauser H, Mischinger HJ, Beham A, Berger A, Cerwenka H, Razmara J, Fruhwirth H, Werkgartner G. Cystic retroperitoneal lymphangiomas in adults. Eur J Surg Oncol. 1997 Aug;23(4):322-6. doi: 10.1016/s0748-7983(97)90777-0. PMID: 9315061.
- Gupta R, Sharma R, Gamanagatti S, Dogra PN, Kumar A. Unilateral renal lymphangiectasia: imaging appearance on sonography, CT and MRI. Int Urol Nephrol. 2007;39(2):361-4. doi: 10.1007/s11255-006-9039-z. Epub 2006 Dec 14. PMID: 17171417.
- Hassanein AH, Mulliken JB, Fishman SJ, Quatrano NA, Zurakowski D, Greene AK. Lymphatic malformation: risk of progression during childhood and adolescence. J Craniofac Surg. 2012 Jan;23(1):149-52. doi: 10.1097/SCS.0b013e3182413ea8. PMID: 22337394.
- Luks VL, Kamitaki N, Vivero MP, Uller W, Rab R, Bovée JV, Rialon KL, Guevara CJ, Alomari AI, Greene AK, Fishman SJ, Kozakewich HP, Maclellan RA, Mulliken JB, Rahbar R, Spencer SA, Trenor CC 3rd, Upton J, Zurakowski D, Perkins JA, Kirsh A, Bennett JT, Dobyns WB, Kurek KC, Warman ML, McCarroll SA, Murillo R. Lymphatic and other vascular malformative/overgrowth disorders are caused by somatic mutations in PIK3CA. J Pediatr. 2015 Apr;166(4):1048-54.e1-5. doi: 10.1016/j.jpeds.2014.12.069. Epub 2015 Feb 11. PMID: 25681199; PMCID: PMC4498659.
- Zenner K, Cheng CV, Jensen DM, Timms AE, Shivaram G, Bly R, Ganti S, Whitlock KB, Dobyns WB, Perkins J, Bennett JT. Genotype correlates with clinical severity in PIK3CA-associated lymphatic malformations. JCI Insight. 2019 Nov 1;4(21):e129884. doi: 10.1172/jci.insight.129884. PMID: 31536475; PMCID: PMC6948764.
- Kashgari AA, Ozair N, Al Zahrani A, Al Otibi MO, Al Fakeeh K. Renal lymphangiomatosis, a rare differential diagnosis for autosomal recessive polycystic kidney disease in pediatric patients. Radiol Case Rep. 2016 Dec 23;12(1):70-72. doi: 10.1016/j.radcr.2016.11.016. PMID: 28228882; PMCID: PMC5310393.
- Restrepo JM, López Amaya JE, Sepúlveda NA, et al. Renal lymphangiectasia MDCT and MRI findings. Rev Colomb Radiol. 2011; 22(3):1-8.
- Riehl J, Schmitt H, Schäfer L, Schneider B, Sieberth HG. Retroperitoneal lymphangiectasia associated with bilateral renal vein thrombosis. Nephrol Dial Transplant. 1997 Aug;12(8):1701-3. doi: 10.1093/ndt/12.8.1701. PMID: 9269653.
- Mani NB, Sodhi KS, Singh P, Katariya S, Poddar U, Thapa BR. Renal lymphangiomatosis: a rare cause of bilateral nephromegaly. Australas Radiol. 2003 Jun;47(2):184-7. doi: 10.1046/j.0004-8461.2003.01149.x. PMID: 12780450.
- Chiu JS, Wu CJ, Sun GH, Lin SH. Obstructive uropathy associated with bilateral renal lymphangiomatosis. Nephrol Dial Transplant. 2004 Nov;19(11):2923. doi: 10.1093/ndt/gfh291. PMID: 15496571.
- Umapathy S, Alavandar E, Renganathan R, S T, Kasi Arunachalam V. Renal Lymphangiectasia: An Unusual Mimicker of Cystic Renal Disease - A Case Series and Literature Review. Cureus. 2020 Oct 8;12(10):e10849. doi: 10.7759/cureus.10849. PMID: 33178504; PMCID: PMC7651773.
- Ashraf K, Raza SS, Ashraf O, Memon W, Memon A, Zubairi TA. Renal lymphangiectasia. Br J Radiol. 2007 Jun;80(954):e117-8. doi: 10.1259/bjr/16931054. PMID: 17684071.
- Kumar N, Yadav P, Ansari MS, Lal H. Surgical management of giant retroperitoneal lymphangioma in a child. BMJ Case Rep. 2020 Feb 13;13(2):e234447. doi: 10.1136/bcr-2020-234447. PMID: 32060118; PMCID: PMC7046380.
- Valerio M, Meuwly JY, Tawadros C, Jichlinski P. Percutaneous drainage and sclerotherapy as definitive treatment of renal lymphangiomatosis. Can Urol Assoc J. 2012 Feb;6(1):E3-7. doi: 10.5489/cuaj.11034. PMID: 22396381; PMCID: PMC3289709.
- Alshanafey S, Alkhani A, Alkibsib A. Renal lymphangiectasia in pediatric population: case series and review of literature. Ann Saudi Med. 2022 Mar-Apr;42(2):139-144. doi: 10.5144/0256-4947.2022.139. Epub 2022 Apr 7. PMID: 35380057; PMCID: PMC8981996.
- Kashgari AA, Ozair N, Al Zahrani A, Al Otibi MO, Al Fakeeh K. Renal lymphangiomatosis, a rare differential diagnosis for autosomal recessive polycystic kidney disease in pediatric patients. Radiol Case Rep. 2016 Dec 23;12(1):70-72. doi: 10.1016/j.radcr.2016.11.016. PMID: 28228882; PMCID: PMC5310393.
- Schwarz A, Lenz T, Klaen R, Offermann G, Fiedler U, Nussberger J. Hygroma renale: pararenal lymphatic cysts associated with renin-dependent hypertension (Page kidney). Case report on bilateral cysts and successful therapy by marsupialization. J Urol. 1993 Sep;150(3):953-7. doi: 10.1016/s0022-5347(17)35660-4. PMID: 8345618.
- Wadhwa P, Kumar A, Sharma S, Dogra PN, Hemal AK. Renal lymphangiomatosis: imaging and management of a rare renal anomaly. Int Urol Nephrol. 2007;39(2):365-8. doi: 10.1007/s11255-006-9002-z. Epub 2006 Sep 27. PMID: 17004034.
- Pollack SF, Geffrey AL, Thiele EA, Shah U. Primary intestinal lymphangiectasia treated with rapamycin in a child with tuberous sclerosis complex (TSC). Am J Med Genet A. 2015 Sep;167A(9):2209-12. doi: 10.1002/ajmg.a.37148. Epub 2015 May 5. PMID: 25943403.
- Dawidek MT, Aquil S, Alogaili R, Gabril M, Moussa M, Sener A, Luke PP. Renal Lymphangiectasia in the Transplanted Kidney: Case Series and Literature Review. Transplantation. 2020 Jan;104(1):172-175. doi: 10.1097/TP.0000000000002745. PMID: 30964839.