
More Information
Submitted: June 21, 2021 | Approved: July 20, 2021 | Published: July 21, 2021
How to cite this article: Lopez JLD, Galindo JF, Villaquiran MR, Valenzuela ED, Cardenas A, et al. Multifrecuency bioimpedance phase angle as a tool to predict maturation failure of native fistulae for hemodialysis. J Clini Nephrol. 2021; 5: 061-066.
DOI: 10.29328/journal.jcn.1001076
Copyright License: © 2021 Lopez JLD, et al. This is an open access article distributed under the Creative Commons Attribution License, which permits unrestricted use, distribution, and reproduction in any medium, provided the original work is properly cited.
Keywords: Chronic kidney disease; Arteriovenous fistula; Phase angle; Multi-frequency bioimpedance

Multifrecuency bioimpedance phase angle as a tool to predict maturation failure of native fistulae for hemodialysis
José Lucas Daza Lopez1*, John F Galindo2, Mónica R Villaquiran3, Emilio D Valenzuela4, Andres Cardenas5, Luis Jose Daza6, Maria Camila Correcha7, Jonathan de Jong8, Yaroslad De La Cruz Prieto9, Gerardo Gutierrez10 and Luis Puello11
1Internist, Nephrologist, Ibague, Colombia Nephrology and Dialysis Unit, Fresenius Medical Care (FMC), Barrio Restrepo Macarena Alta calle, 41 #5-40, Ibagué 73001, Colombia
2General Medicine Ibague, Colombia
3Nutrition Ibague, Colombia
4Intensive Care, Epidemiologist, Santiago, Chile
5Medical Student Santa Marta, Colombia
6Internist, Hematologist Cartagena, Colombia
7Medical Student, Manizales, Colombia
8Medical Student, Manizales, Colombia
9Internist, Nephrologist, Cali, Colombia
10Internist, Nephrologist, Villavicencio, Colombia
11Internist, Nephrologist, Cartagena, Colombia
*Address for Correspondence: Jose Lucas Daza Lopez, Internist, Nephrologist, Ibague, Nephrology and Dialysis Unit, Fresenius Medical Care (FMC), Barrio Restrepo Macarena Alta calle 41 #5-40, Ibagué 73001, Colombia, Email: [email protected]
Background and objectives: An arteriovenous fistula is considered to be an ideal vascular access for patients receiving hemodialysis, its main limitation is its high failure rate to achieve maturation and long-term functionality loss. Multiple strategies have attempted to identify patients at risk. Bioelectrical impedance has shown to be a valuable resource in the determination of the hydration status, and the measurement of the phase angle through this method has demonstrated to be a good indicator of the nutritional state and its related as a general marker of survival. The objective of this study is to analyze the role of plasma albumin and phase angle measured through bioelectrical impedance as tools useful for predicting failure of arteriovenous fistulas.
Materials and methods: prospective observational study, including 104 patients with chronic kidney disease receiving hemodialysis who underwent a native arteriovenous fistula during a period of 24 months. Analyzing its clinical characteristics, laboratory and phase angle through electrical bioimpedance, both univariate and multivariate analysis was performed both with logistic regression, furthermore calculation of coordinates and ROC curve to establish a better cut-off point.
Results: of the variables that were analyzed only the phase angle measurement showed statistical significance OR 2.61 (1.6 – 4.4) p - value 0.001 for predicting arteriovenous fistula failure. In female patients with a phase angle value of 3.25 had a 90% sensibility and 53% specificity for male patients a value of 3.58 showed a sensibility of 84% and a specificity of 52% with ROC curve of 0.78.
Conclusion: phase angle through bioimpedance is a useful parameter, helpful in predicting failure of native arteriovenous fistula, it is also an important tool for identifying patients at risk, in early stages prior to the construction of a vascular access.
Native arteriovenous fistulas are considered to this date to be the vascular access of choice widely recommended to patients undergoing chronic hemodialysis, due to its advantages, such as its cost-benefit relation, longer duration, lower rate of infection, hospital admission and mortality [1,2].
However, its main inconvenience, is the failure or loss of the vascular access, depending on the series this can be around 60% in the first and includes primary failure presenting within the first 72 hours after its constructions as well as loss of functionality which is described as an impossibility of achieving an adequate dialytic treatment after 6 or 8 weeks with maturation two needle techniques, representing an important cause of morbidity, hospital admission and an increase in healthcare costs [3-5].
Various factors have been identified to this date related with the failure of establishing a vascular access, some in a clearer manner than other, however none of these factors has shown a relevant role in an isolated manner[6-8].
Within the multiples factors identified and those which possible adverse association with an arteriovenous fistula is still unknown among these is the nutritional status [9,10], currently known as protein-energy wasting syndrome, its association with cardiovascular risk and mortality in patients undergoing hemodialysis [9-12]. The relation between malnutriton and adverse surgery results in terms of complications, days of hospital stay, infection and mortality [13], however its association with adverse results in arteriovenous fistulas has not been demonstrated, partially due to difficulties in defining its criteria, among the tools used for its quantification and the use of biological and biochemical markers such as albumin which presents important limitations in patients undergoing hemodialysis.
Recently, electrical bioelectrical impedance has become a valuable tool in the area of nephrology, this is based on the fact that biological systems due to their composition of electrolytes and cellular membranes with specific polarities are considered conductors of electrical current [14,15]. Bioelectrical impedance is a technique which determines the opposition of an organism as an alternating current passes through, giving a measurement of impedance (Z) which is the result of two components: the resistance presented when a current passes through which is represented by the content of body water and its reactance which reflects the capacity of cells to store electrical energy (serving as condensers) in theory this correlates with the integrity of a cellular membrane. The two components, the resistance (R) which reflects the hydration status and the reactance (Xc) which indicates the nutritional status are represented as a vector and reflects the body water and cellular integrity respectively; the angle resulting from these two measurements is known as the phase angle (PA) which in eutrophic patients with no nutritional deficit has a value inferior to 10 degrees and has been consistently related with nutritional status [17-19].
Bioimpedance allows the calculation of body composition in terms of percentages of fat tissue and lean tissue, its hydration status in terms of a percentage of hydration in relation to intra- and extracellular liquid, which has allowed for a more precise quantification of nutritional status and dry weight [18-20].
The phase angle is considered to be a measurement of cellular stability and integrity that has a well-defined correlation with nutritional status and is considered to be an important predictor of survival in patients with chronic kidney disease compared with other traditionally used determinations such as DEXA (Dual energy X-ray absorptiometry assessment), global subjective evaluation and biochemical markers like total proteins and albumin; and its relation with mortality in this population has been described [21-23] (Figure 1).
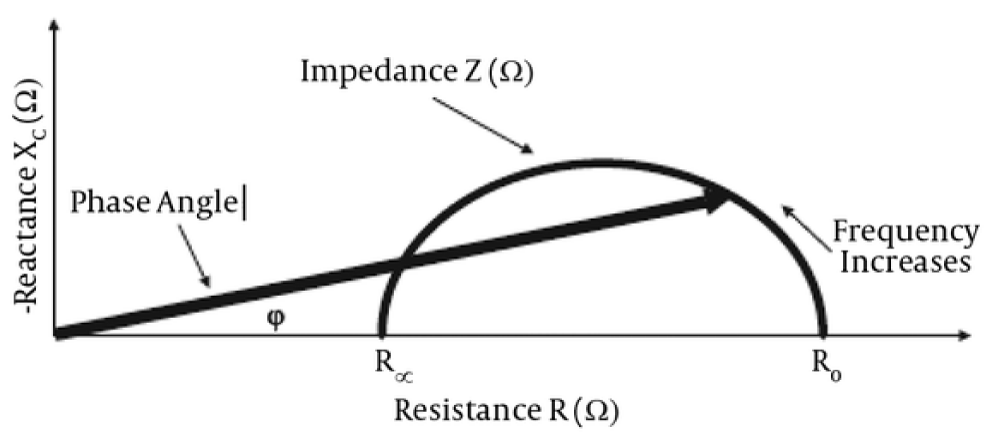
Figure 1: Phase angle from bioelectrical impedance.
To this date only few studies have taken into account the relation between plasma albumin levels and adverse results related to arteriovenous fistulas, suggesting that low levels of plasma albumin could associate with failure of maturation of native fistulas [24,25], however, considering that albumin is not an ideal marker for evaluating nutritional status in patients undergoing hemodialysis, its role as a tool helpful in predicting the probability of success or failure of a vascular access like an arteriovenous fistula is still unclear.
The objective of this study is to evaluate the performance of plasma albumin, phase angle through multi-frequency bioimpedance and its value as a potential predictor of failure in arteriovenous fistulas for hemodialysis and establish if malnutrition determined through this behaves as a new risk factor for adverse results related to vascular access.
Baseline patients characteristics
Initially, 109 patients from a single Colombian dialysis center who were subjected to native FAV construction at the discretion of the vascular surgeon of the dialysis center were recruited, both proximal and distal fistulas were included during de follow-up period and met the inclusion criteria. The information from five patients was not included in the final analysis, a patient carrying pacemaker who did not allow reliable bio impedance data, four lost, 3 cardiovascular death and a loss of tracking. Finally, 104 patients were included for the corresponding statistical analysis. It is not possible to stablish comparison groups as to date there is not a gold standard reference test for vascular access failure detection at the pre-operative stage (Figure 2).
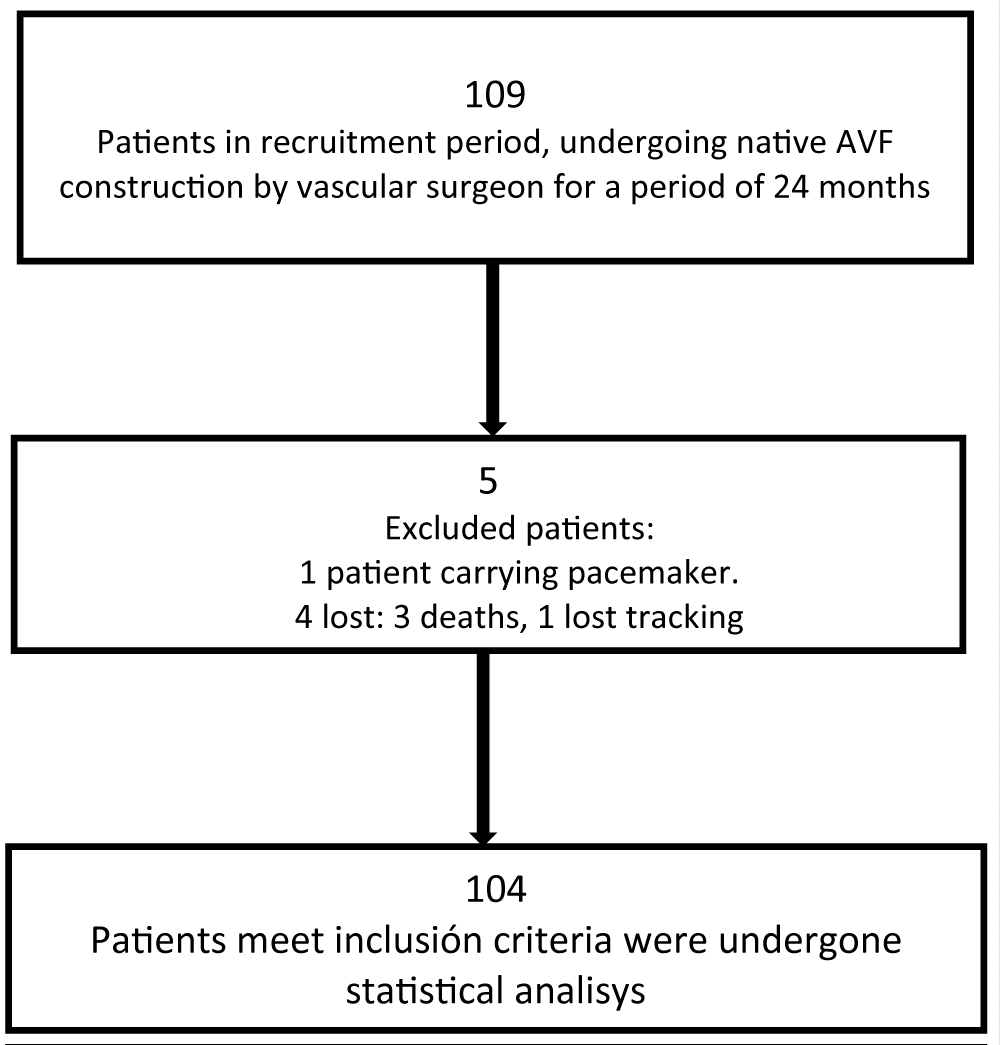
Figure 2: Flow Chard of study population.
An observational prospective study was realized during a period of 24 months, patients with CKD G5 defined by KDOQI 2002 criteria, which underwent chronic hemodialysis three times per week and 4 hours duration per dialysis session, Biochemical parameters were taken at the beginning of the dialysis session such as hemoglobin, parathyroid hormone, ferritin, plasma albumin, urea nitrogen, serum electrolytes.
Analyzing demographical characteristics, laboratory variables, associated comorbidities and phase angle at 50 kHz (PA50) measured by multi-frequency bioimpedance using a spectroscopic bioimpedance machine. (BCM - Fressenius Medical Care D GmbH). As a protocol measure in the institution, bioimpedance is performed when the patient is admitted to the renal unit classified as chronic kidney disease and monthly follow-up
On a total of 104 patients.
Inclusion criteria: Patients prevalent in hemodialysis, more than 90 days undergoing dialysis, patients over the age of 18 years undergoing construction of a native arteriovenous fistula,
Exclusion criteria: Patients who underwent construction of a native arteriovenous fistula but didn’t have their complete data registered, patients who passed away during the data recollection period (Table 1).
| Table 1: Demographic characteristics | ||
| n 104 | Absolute frequency | Percentage |
| Female | 73 | 70,2% |
| Male | 31 | 29,8% |
| Diabetes | 60 | 57,7% |
| HTA | 101 | 97.1% |
| PAD | 44 | 42,3% |
| CVC | 99 | 95.2% |
| HTA: Arterial Hypertension; CVC: Central Venous Catheter; PAD: Peripheral Artery Disease | ||
The data and variables related to laboratory were obtained from clinical electronic registers corresponding to the period during the construction of the arteriovenous fistula, which was performed by a vascular surgeon experienced in the construction of vascular access destined for hemodialysis. Bioimpedance measurements were taken by the nutrition group, according to specification of the dialysis center; prior to starting dialytic treatment with the patient a supine position, electrodes were placed on the arm and leg of the same side of the body; following recommendations made by its manufactures to assure standardization of all measurements. The 50 kHz phase angle determinations were obtained through a data storage card included in the bioimpedance device and its incorporated program Fluid Manager Tool (FMT Fressenius Medical Care) and the electronic clinical register during the evaluation performed by the nutrition group prior to the surgical procedure. Bioimpedance measurements were made at the beginning and at one month with the sequential intake on 3 occasions and the average value was used (Table 2).
| Table 2: Analytical laboratory variables | |
| n 104 | Mean - SD |
| Hb (mg/dl) | 10 ± 1,83 |
| BMI | 23.1 ± 4,2 |
| Age (Years) | 62 ± 14 |
| Ferritin (ng/ml) | 591 ± 429 |
| Phase angle(F) | 3,57 ± 1,07 |
| Phase angle(M) | 4,27 ± 1,25 |
| PTH (nmol/l) RIQ | RIQ 25: 157 RIQ 75: 395 |
| Albumin (gr/dl) RIQ | RIQ 25: 3,79 RIQ 75: 4,1 |
| HB: Hemoglobin: BMI: Body Mass Index; IQR: Interquartile Range; PTH: Parathyroid Hormone | |
The maturation criterion used in the study was the use of the fistula with two needles in 75% of the sessions during a time interval of 4 weeks, with blood flow administered by the dialysis machine of 300 ml / min (at least 4 continuous sessions) or 1.4 ktv or a urea reduction rate of 70% (it was not possible to use ultrasound-Doppler measurements due to lack of equipment and economic deficit). During the follow-up, the moment of prior evaluation is documented by a nursing group the successful or not puncture of the fistula, considering a functional maturation when a fistula is successfully and effectively cannulated with a two-needle method which allows for dialytic treatment with adequate flow and pressures therefore a non-successful fistula is one that doesn’t allow to be punctured, those that presented primary failure and those that required another vascular access for dialytic treatment within 12 weeks of its construction.
Statistical analysis
SPSS version 20.0 software was used for the statistical analysis of patients that presented primary failure in the process of functional maturation of the vascular access as primary result as was defined within the materials and methods section and its relation with the phase angle and serum albumin concentration.
The Kolmogorov Smirnov test was applied to define the distribution of variables; the parametric variables were represented as a mean average and standard deviation and non-parametric variable as median and interquartile ranges. Univariate logistic regression analysis was performed on variables of interest for predicting failure of vascular access. Including dependent variables which showed statistical significance for the subsequent multivariate analysis. Area under the curve was obtained and a cut-off point was determined with the highest sensibility and specificity for predicting failure of fistula by phase angle. Statistical significance was set at p < 0.05.
Of 104 individuals followed during the development of this study a 32.2% achieved a successful maturation of the fistula which allowed for optimal dialytic treatment; in the remaining 67.8% of individual an adequate vascular access was not achieved, which is similar to data described in current literature. Of this last group the records of 73 male participants (70.2%), 31 female participants (29.8%) with a mean age of 62 years (SD: 14 years) 57.7% of all patients were diabetic, 97.1% had hypertension, 42.3% with a background of peripheral artery disease. 92.5% of the studied population had a central venous catheter at the moment of construction of the arteriovenous fistula (Table 1).
Among the analytical variables presented were hemoglobin, ferritin and phase angle for males as well as females (Table 2); measurements were of frequency in terms of its median and respective standard deviations. For plasma albumin and parathyroid hormone its means and measurements of tendency were described in terms of interquartile ranges set at 25 and 75 respectively.
Univariate analysis for measurements of parathyroid hormone and ferritin did not show any association with the primary event evaluated. Similar findings were obtained for measurements of hemoglobin and body mass index.
Cut-off points were established for phase angle in female patients at 3.25 with a sensibility of 90% and specificity 53%; and for males’ phase angle at 3.58 for a sensibility of 84% and specificity of 52% with an area under the curve of 0.78 (Figure 3).
Figure 2: Phase angle from bioelectrical impedance.
The binary logistic regression analysis for plasma and phase angle variable only showed statistical significance for the latter one in the evaluation of the primary objective (Table 4).
| Table 2: Analytical laboratory variables | |
| n 104 | Mean - SD |
| Hb (mg/dl) | 10 ± 1,83 |
| BMI | 23.1 ± 4,2 |
| Age (Years) | 62 ± 14 |
| Ferritin (ng/ml) | 591 ± 429 |
| Phase angle(F) | 3,57 ± 1,07 |
| Phase angle(M) | 4,27 ± 1,25 |
| PTH (nmol/l) RIQ | RIQ 25: 157 RIQ 75: 395 |
| Albumin (gr/dl) RIQ | RIQ 25: 3,79 RIQ 75: 4,1 |
| HB: Hemoglobin: BMI: Body Mass Index; IQR: Interquartile Range; PTH: Parathyroid Hormone | |
As far as known, this is the first study designed to attempt establish if phase angle measurement through bioimpedance predicts maturation failure of arteriovenous fistulas. Within the studied population we evaluated clinical characteristics, traditional variables, plasma albumin, and phase angle; this last one showed statistical significance within the evaluation of the primary objective (Table 3).
| Table 3: Univariate analysis of predictors for primary failure in arteriovenous fistula | ||
| n 104 | OR (CI 95%) | p value |
| Hb (mg/dl) | 1,06(0,86-1,31) | 0,55 |
| Ferritin (ng/ml) | 1,09(0,99-1.01) | 0,78 |
| PTH(nmol/l) | 1,00(0,99-1,00) | 0,72 |
| Albumin (gr/dl).log | 13,7(1,3-137,3) | 0,026 |
| BMI | 1,04(0,95-1,14) | 0,368 |
| Phase angle | 2,69(1,71-4,23) | 0,001 |
| HB: Hemoglobin: BMI: Body Mass Index; PTH: Parathyroid Hormone | ||
| Table 4: Binary logistic regression for predicting failure of arteriovenous fistula | ||
| Variables | OR (CI 95) | p value |
| Phase angle | 2,61(1,66-4,1) | 0.001 |
| Albumin (gr/dl) | 3,31(0,30-30) | 0,34 |
Failure of establishing vascular access remains a frequent cause of morbidity and elevated healthcare costs for patients undergoing hemodialysis; investigation of such determinants of vascular access maturation failure will have direct implications on the care these patients receive. Due to identifying patients at risk of vascular access failure being of capital importance, efforts must be directed towards the search of more objective ways of predicting; current guidelines focusing on preventing vascular access failure seek to identify the patients with most risk factors, complete physical examination, use of biochemical parameters and adequate imaging resources.
Plasma albumin is one of the biochemical parameters used as a nutritional measure and a tool that allows the diagnosis of malnutrition or malnutrition or loss of caloric proteins and, like other published studies, it is correlated with worse results at the time of the construction of an arteriovenous fistula , but insufficient from a clinical point of view because despite the fact that plasma albumin is still measured in previous studies and in daily clinical practice, the results are scarce to try to predict the failure of arteriovenous fistulas.
In this study, it was shown that the bioimpedance phase angle is superior to albumin in predicting failure in arteriovenous fistulae, in addition, another advantage offered by the bioimpedance phase angle is its low cost, rapid operation, little technical difficulty and its non-functional nature. invasive qualify it as one of the recommended methods to estimate body composition and more in this population of patients with chronic kidney disease on hemodialysis where protein caloric loss is more accentuated with greater morbidity and mortality, and they use only albumin as a parameter.
Nutritional is insufficient because its result is subject to multiple variations due to the clinical conditions of these patients.
That is why the phase angle becomes a useful tool not only as a predictor in the failure of arteriovenous fistulas but also as one of the most recommended methods at present to measure body composition and better discriminate nutritional status.
Our study suggests that the measurement of phase angle through multifrequency bioimpedance at 50 kHz, with cut-off values of 3.25 for female patients and 3.58 for male patients, it presents a significant association with adverse results in fistulas for hemodialysis in terms of primary failure and/or failure to achieve functional maturation; This finding could be explained by the relationship between the low phase angle and malnutrition in patients in dialysis as reported by other authors, Which lead us to infer that the poor nutritional status could be an independent risk factor for the development of adverse results after the construction of native hemodialysis fistulas.
Although our study is not designed to establish the role of specific mechanisms that explain the failure vascular access, if it allows for better selection of patients at the highest risk of failure in the pre-operative period order to stablish interventions measures of potentially modifiable factors such as nutritional status and preserve the vascular beds of them in whom the risk fails to achieve maturation is high.
We conclude that phase angle measured through bioimpedance, could be a useful tool to be considered in the identification of patients at risk of native fistula for dialysis maturation failure during the pre-surgical stage.
Bioimpedance integrates measurements of various body segments with variable physical effects such as hydration status, fatty tissue percentage, lean tissue and percentage of total body water and given low phase angle values are associated with worse nutritional conditions and worse prognostics additional investigations are required that allow defining if malnutrition can behave as a new risk factor for adverse results related to fistulas to account for.
To date, references test for prediction of access failure in the preoperative stage are lacking, so it was not possible to establish our groups of study without comparison; This work opens the possibility of future research to make use of the emergent tools and technologies for use by the vascular surgeon and nephrologists as a part of clinical daily practice for preoperative evaluation the patients in whom the construction of native hemodialysis fistulas is planned.
Difficulties in validation bioimpedance in different ethnic groups, variability in clinical conditions and abnormal hydration status have led to a large quantity of equations which can be of difficult interpretation and application within the context of the studied population.
Ethical responsibilities
Protection of persons and animals. The authors declare that for this investigation no experiments were performed on humans nor animals.
Confidentiality of data: The authors declare that they have followed the protocols related to patient data publishing as established by their work place.
Availability of data and materials: The data and materials were all included in the manuscript
Authors’ contributions: Jose Lucas Daza (JLD) is responsible for the writing of the manuscript. JLD performed the acquisition and interpretation of data and drafted and revised the manuscript. All authors read and approved the final manuscript.
Ethics approval and consent to participate: Written informed consent was obtained from the patient for publication of this manuscript, and the accompanying images were auditioned at the bibliographic references. This study/report was approved by the Ethical Committee of the Fresenius Medical Care and was conducted in accordance with the National Law on the protection of personal data No 25.326 and the Declaration of Helsinki (Last version, Fortaleza 2013).
Consent for publication: Written informed consent was obtained from the patient for publication of this manuscript, and the accompanying images were auditioned at the bibliographic references.
- Ronald PL, Charlotte AJ, Justin AM, Ethier J, Kimata N, et al. Facility hemodialysis vascular access use and mortality in countries participating in DOPPS: an instrumental variable analysis. Am J Kidney Dis. 2009; 53: 475-491. PubMed: https://pubmed.ncbi.nlm.nih.gov/19150158/
- Pietro R, Suetonia PC, Matthew OJ, Quinn RR, MacRae JM, et al. Associations between hemodialysis access type and clinical outcomes: a systematic review. J Am Soc Nephrol. 2013; 24: 465-473. PubMed: https://pubmed.ncbi.nlm.nih.gov/23431075/
- Damian MG, Alexander MP, Aurang KZ, Nicolas IG. Current tools for prediction of arteriovenous fistula outcomes. Clin Kidney J. 2015; 8: 282-289. PubMed: https://pubmed.ncbi.nlm.nih.gov/26034589/
- Brian BD, Rachel FB, Albert AM, Anthony MS, Critchlow CW, et al. Predictors of early mortality among incident US hemodialysis patients in the Dialysis Outcomes and Practice Patterns Study (DOPPS). Clin J Am Soc Nephrol. 2007; 2: 89-99. PubMed: https://pubmed.ncbi.nlm.nih.gov/17699392/
- Mahmoud MB, Joseph CK, Caitlin HW, Arhuidese IJ, Zarkowsky DS, et al. Trends in incident hemodialysis access and mortality. JAMA Surg. 2015; 150: 441-448. PubMed: https://pubmed.ncbi.nlm.nih.gov/25738981/
- Vascular Access Work Group. Clinical practice guidelines for vascular access. Am J Kidney Dis. 2006; 48: S248–S273. PubMed: https://pubmed.ncbi.nlm.nih.gov/16813991/
- Wells AC, Fernando B, Butler A, Huguet E, Bradley JA, et al. Selective use of ultrasonographic vascular mapping in the assessment of patients before haemodialysis access surgery. Br J Surg. 2005; 92: 1439-1443. PubMed: https://pubmed.ncbi.nlm.nih.gov/16187267/
- George SE, Risha G, Ian CC. Factors affecting the patency of arteriovenous fistula for dialysis access. Review Articles. J Vasc Surg. 2012; 55: 849-855. PubMed: https://pubmed.ncbi.nlm.nih.gov/22070937/
- Tammy H, Ranil DN, Desilva PK, Vin Y, Brown RS, et al. Factors predicting failure of AV ‘fistula first’ policy in the elderly. Hemodial Int. 2014; 18: 507-515. PubMed: https://pubmed.ncbi.nlm.nih.gov/24400842/
- Wong V, Ward R, Taylor J, Selvakumar S, How TV, et al. Factors associated with early failure of arteriovenous fistulae for haemodialysis access. Eur J Vasc Endovasc Surg. 1996; 12: 207-213. PubMed: https://pubmed.ncbi.nlm.nih.gov/8760984/
- Charmaine LE, Michael A, Louise M, Matthew OJ, et al. Risk Equation Determining Unsuccessful Cannulation Events and Failure Maturation in Arterio Venous Fistulas. JASN. 2006; 17: 3204-3212. PubMed: https://pubmed.ncbi.nlm.nih.gov/16988062/
- Gracia-Iguacel C, González-Parra E, Barril-Cuadrado G, Sánchez R, Egido J, et al. Defining protein-energy wasting syndrome in chronic kidney disease: prevalence and clinical implications. Nefrologia. 2014; 34: 507-519. PubMed: https://pubmed.ncbi.nlm.nih.gov/25036065/
- Maggiore Q, Nigrelli S, Cicarelli C, Grimaldi C, Rossi GA, et al. Nutritional and prognostic correlates of bioimpedance indexes in hemodialysis patients. Kidney Int. 1996; 502: 2103-2108. PubMed: https://pubmed.ncbi.nlm.nih.gov/8943496/
- Louis M, Alexandrine O, Melissa B, Trnkus A, Ouimet MA, et al. Phase Angle as Biomarker for Frailty and Postoperative Mortality: The BICS Study. J Am Heart Assoc. 2018; 7: e008721. PubMed: https://pubmed.ncbi.nlm.nih.gov/30371163/
- López-Gómez JM. Evolution and aplications of bioimpedance in managing chronic kidney disease. editorial comments. Nefrologia. 2011; 31: 630–634. PubMed: https://pubmed.ncbi.nlm.nih.gov/22130276/
- Dumler F, Kilates C. Use of bioelectrical impedance techniques for monitoring nutritional status in patients on maintenance dialysis. J Renal Nutr. 2000; 10: 116–124. PubMed: https://pubmed.ncbi.nlm.nih.gov/10921532/
- Nescolarde L, Picoli A, Roman A, Nuñez A, Núñez A, Morales R, et al. Bioelectrical imedance vector analysis in haemodialysis patients: relation between oedema and mortality. Physiol Meas. 2004; 25: 1271-1280. PubMed: https://pubmed.ncbi.nlm.nih.gov/15535191/
- Ursula KG, Ingvar B, Antonio D, Paul D, Elia M, et al. Bioelectrical Impedancy analysis part I: Review of principles and methods. Clin Nutr. 2004; 23: 1226-1243. PubMed: https://pubmed.ncbi.nlm.nih.gov/15380917/
- Ursula KG, Ingvar B, Antonio D, Paul D, Elia M, et al. Bioelectrical Impedancy analysis part II: Utilization in clinical Practice. Clinical Nutrition. 2004; 23: 1226-1243. PubMed: https://pubmed.ncbi.nlm.nih.gov/15380917/
- Laurynas R, Alvita G, Vaidas V, Jelena P, Marius M. Malnutrition assessment in hemodialysis patients: Rol of bioelectrical Impedance analysis phase angle. J Renal Nutr. 2016; 26: 391-395. PubMed: https://pubmed.ncbi.nlm.nih.gov/27450205/
- Francisco C, Coral MD, Juan V, Rocio GM, Flavio F. Hydration status assessment by multi-frecuency bioimpedance in patients with advanced chronic kidney disease. Nefrologia. 2011; 31: 537–544. PubMed: https://pubmed.ncbi.nlm.nih.gov/21959720/
- Antje F, Andrew D. Comparision Of Multifrecuency Bioelectrical Impedance Analisis And Dual Energy X ray Absrptiometry Assessment in Outpatients Hemodialisis Patients. Am J Kidney Dis. 2010; 57: 123-129. PubMed: https://pubmed.ncbi.nlm.nih.gov/20692749/
- Donata R, Dalia G, Vaidas V, et al. Malnutrition assessed by phase angle determines outcomes in Low – risk cardiac surgery patients. Clinical Nutrit. 2016; 35: 1328-1332. PubMed: https://pubmed.ncbi.nlm.nih.gov/26935019/
- Jung-Ho S, Chae KR, Ki PH, Jin HH, Su KH. Predicting clinical outcomes using Phase Angle as assessed by bioelectrical impedance in maintenance hemodialysis patients. Nutrition. 2017; 41: 7-13. PubMed: https://pubmed.ncbi.nlm.nih.gov/28760431/
- Vedran P, Tvrtko H, Josip P, Zimak Z, Hauptman D, et al. Hypoproteinemia as a prognostic risk factor for arteriovenous fistula failure. Hemodialysis Int. 2018; 22: 37-44. PubMed: https://pubmed.ncbi.nlm.nih.gov/28133903/
- Ali K, Evripidis T, Alan A, Mekhola H, Yiannis P. The independent association of preoperative serum albumin on the functional maduration of radiocephalic arteriovenous fistulae. J Vasc Access. 2017; 18: 148-152. PubMed: https://pubmed.ncbi.nlm.nih.gov/28127727/
- Tammy H, Ranil DN, Bhanu PK, Yael V, et al. Factors predicting failure of AV ‘fistula first’ policy in the elderly. Hemodial Int. 2014; 18: 507-515. PubMed: https://pubmed.ncbi.nlm.nih.gov/24400842/
- Maggiore Q, Nigrelli S, Ciccarelli C, Grimaldi C, Rossi GA, et al. Nutritional and prognostic correlates of bioimpedance indexes in hemodialysis patients. Kidney Int. 1996; 50: 2103-2108. PubMed: https://pubmed.ncbi.nlm.nih.gov/8943496/